Download
1 / 49
800 likes | 1.53k Vues
MANAGEMENT OF ADOLESCENT PCOS. DR.ABHISHEK SINGH PARIHAR M.S ( Obs & Gyne ) ; FELLOW REPRODUCTIVE MEDICINE CONSULTANT : LIFECARE IVF CENTRE, NEW DELHI ABALONE CLINIC, NOIDA

E N D
MANAGEMENT OF ADOLESCENT PCOS DR.ABHISHEK SINGH PARIHAR M.S (Obs & Gyne) ; FELLOW REPRODUCTIVE MEDICINE CONSULTANT : LIFECARE IVF CENTRE, NEW DELHI ABALONE CLINIC, NOIDA ETERNA IVF CENTER, NEW DELHI
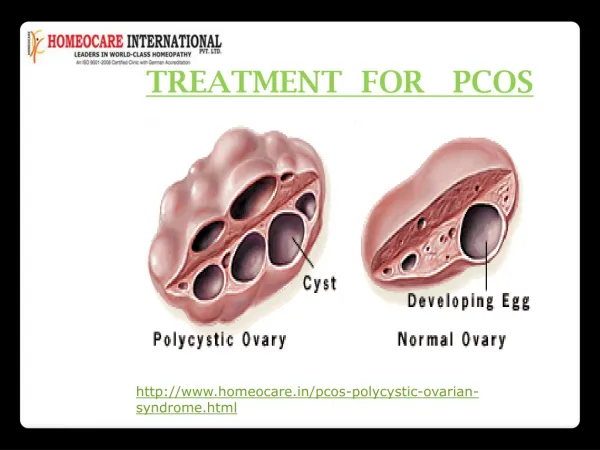
DEFINITION • PCOS is a heterogenous endocrine metabolic disorder characterised by hyperandrogenemia,chronic anovulation,and/or polycystic ovaries • Irving F.Stein & Michael L. Leventhal -1935
MAIN FEATURES -Anovulation -POLYCYSTIC OVARIES -Hyperinsulinemia -Hyperandrogenism
Rotterdam consensus Revised 2003 criteria (2 out of 3) 1. Oligo- or anovulation, 2. Clinical and/or biochemical signs of hyperandrogenism, 3. Polycystic ovaries and exclusion of other etiologies (congenital adrenal hyperplasia, androgen-secreting tumors, Cushing’s syndrome)
Exclusion of related disorders CAH-Basal morning 17-OHP,(2-3 ng/ml) WHO I &III –FSH,LH,E2 Hypothyroidism,Hyperprolactenemia-Sr.TSH,Sr.Prl Syndromes of severe insulin resistance(HAIRAN syn) Cushing syndrome-Dexa supression test Androgen secreting tumours /exogenous androgens
Clinical Presentation Adolescent Period Reproductive Period Menopausal • Menstrual • Irregularity • Obesity • Cosmetic concerns • Acne • Hirsutism Hair Loss • Infertility • Early Pregnancy loss • During pregnancy • PIH • GDM • Metabolic • Syndrome • Ca Endometrium
PCOS Most frequent endocrine problem in adolescent age group In 5-15%women of reproductive age group (12-45 years) Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertility and Sterility Vol. 97, No. 1, January 2012. Bart C. J. M. Fauser et.al.
Life Style Management Diet + Exercise = Weight Loss
Diet Dietary intervention ( high protien, low carbohydrate , low fat diet more effective) Energy deficit of 500-1000 Kcal/day
Diet counselling Goals – practical,realistic,achievable Small frequent meals More fruits/vegetables/fibre(bran) Decreased sugar/fried food /cola Switch to healthy oils More steamed /grilled cooking
Exercise • American Diabetes Association recommends minimum of :- • 150 minutes/week of moderate to vigrous exercise • for individuals with IGT. • Should be distributed over 3 days • For long term weight reduction – 1 hour/day of • exercise is recommended. Ref : Kathleen Metal Clin Obst Gynecol 2007
Role of weight loss 5-7% wt. Reduction effective in restoring normal menses and fertility Ref : Kathleen M et al Fertility & Sterility 2004
50 % by just weight control PCOS can’t be cured but the symptoms can be managed
Consensus on women’s healthaspects of polycystic ovary syndrome(PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOSConsensus Workshop 2010 Fertility and Sterility, Vol. 97, No. 1, January 2012
Overall, the benefits of OCPs outweigh the risks in most patients with PCOS (level B). • Women with PCOS are more likely to have contraindications for OCP use than normal women (level C).
There is no evidence for differences in effectiveness and risk among the various progestogens and when used in combination with a 20 versus 30 mg daily dose of estrogen (level B).
PCOS is a major risk factor for developing IGT and Type 2 Diabetes (level A). • Obesity (by amplifying insulin resistance) is an exacerbating factor in the development of IGT and T2D in PCOS (level A). • The increasing prevalence of obesity in the population suggests that a further increase in diabetes in PCOS is to be expected (level B). • Screening for IGT and T2D should be performed by OGTT (75 g, 0- and 2-hour values). There is no utility for measuring insulin in most cases (level C).
Screening should be performed in the following conditions: hyperandrogenism with anovulation, acanthosis nigricans,obesity (BMI >30 kg/m2, or >25 in Asian populations), in women with a family history of T2D or GDM (level C). • Metformin may be used for IGT and T2D (level A). Avoid use of other insulin sensitizing agents such as thiazolidinediones (GPP).
Prolonged (>6 months) medical therapy for hirsutism is necessary to document effectiveness (level B) • Antiandrogens should not be used without effective contraception (level B) • Flutamide is of limited value because of its dose-dependent hepatotoxicity (level B). • Drospirenone in the dosage used in some OCPs is not antiandrogenic(level B).
There are moderate quality data to support that women with PCOS have a 2.7-fold (95% confidence interval [CI],1.0–7.3) increased risk for endometrial cancer. (level B). Limited data exist that do not support the conclusion that women with PCOS are at increased risk for ovarian cancer (level B).
Limited data exist that do not support the conclusion that women with PCOS are at increased risk for breast cancer (level B).
CONCLUSION • Management of the disease begins by building positive, supportive relationship with adolescent diagnosed with PCOS. • Positive relationship helps adolescent to share the signs and symptoms of this chronic disease which can have great impact on one’s body Image and self esteem… • Dedicated Adolescent health clinics
Implications of diagnosis at adolescent age Optimization of lifestyle Regular metabolic screening Proactive fertility planning with consideration of planning for conception at an earlier age