Download
1 / 66
670 likes | 987 Vues
Closed Fractures of the Tibial Diaphysis. Much emphasis to High Energy fractures In Fact: 76.5% are closed 53.5% have mild soft tissue damage. Tibial Fractures. Most common long bone fracture 492,000 fractures yearly Average 7.4 day hospital stay 100,000 nonunions per year.

E N D
Much emphasis to High Energy fractures In Fact: 76.5% are closed 53.5% have mild soft tissue damage
Tibial Fractures • Most common long bone fracture • 492,000 fractures yearly • Average 7.4 day hospital stay • 100,000 nonunions per year
History & Physical • Pain, inability to bear weight, and deformity • Local swelling and edema variable • Careful inspection of soft tissue envelope, including compartment swelling • Thorough neurovascular assessment including motor/sensory exam and distal pulses
Physical Exam • Soft tissue injury with high-energy crush mechanism may take several days to fully declare itself • Repeated exam to follow compartment swelling
Radiographic Evaluation • AP and Lateral views of entire tibia from knee to ankle • Oblique views can be helpful in follow-up to assess healing
Associated Injuries • Up to 30% of patients with tibial fractures have multiple injuries • Ipsilateral fibula fracture common • Ligamentous injury of knee with high energy tibia fractures • Browner and Jupiter, Skeletal Trauma, 3rd Ed
Associated Injuries • Ipsilateral femur fx, “floating knee” • Neuro/vascular injury less common than in proximal tibia fx or knee dislocation • Foot and ankle injury
Classification • Numerous classification systems • Important variables • Pattern of fracture • location of fracture • comminution • associated fibula fracture • degree of soft tissue injury
OTA Classification • Follows Johner & Wruh system • Relationship between fracture pattern and mechanism • Comminution is prognostic for time • to union Johner and Wruhs, Clin Orthop 1983
Henley’s Classification • Applies Winquist & Hansen grading of femur to fractures of the tibia
Tscherne Classification of Soft Tissue Injury • Grade 0- negligible soft tissue injury • Grade 1- superficial abrasion or contusion • Grade 2- deep contusion from direct trauma • Grade 3- Extensive contusion and crush injury with possible severe muscle injury, compartment syndrome
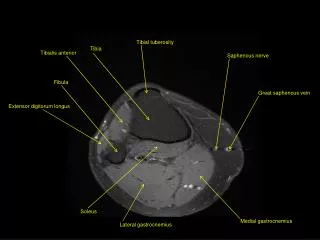
Compartment Syndrome • 5-15% • HISTORY Hi-Energy Crush • 4 leg compartments
Nerve is the Tissue most Sensitive to Ischemia • PAIN first Symptom • PAIN with Passive Stretch first Sign
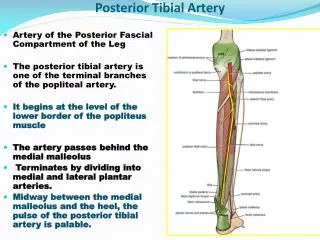
Each Compartmenthas Specific Innervation • Ant Comp - Deep Peroneal N. • Lateral - Sup Peroneal N. • Deep Post. - Tibial N. • Sup Post. - Sural N.
Anterior Compartment • Dorsiflexes ankle • Tib ant, EDL, EHL, and peroneus tertius muscles • Anterior tibial a./v. • deep peroneal n. • 1st webspace sensation
Lateral Compartment • Everts the foot • Peroneus brevis and longus muscles • Superficial peroneal n. dorsal foot sensation
Superficial Posterior Compartment • Plantarflexes ankle • Gastrocnemius, soleus, popliteus, and plantaris muscles • Sural nerve • Lateral heel sensation • Greater and lesser saphenous veins
Deep Posterior Compartment • Plantarflexion and inversion of foot • FDL, FHL, Tib post muscles • Post tibial vessels, peroneal a. • tibial nerve • Plantar foot sensation
Pressure Measurements are Helpful • Various Thresholds P = 30 P = 45 ∆ P < 30 = Diastolic BP - Compartment Pressure McQueen, JBJS-B, 1990
Highest at Fracture Site Highest Pressures in Posterior & Anterior Compartments Pressures Not Uniform +++ ++ + • Heckman JBJS 76
Clinical Monitoring • Need Close Observation • Repetitive Exams • Some instances repetitive Pressure measurements • Indwelling Monitors?
Goals of Fasciotomy • Decompress The Compartment • Do Not Strip Muscle From The Bone • Single vs. Two incisions • Plan for fracture fixation • Plan for wound closure
Closed Tibial Shaft Fractures • Broad Spectrum of Injures w/ many treatments • Nonsurgical management • Intramedullary nails • Plates • External Fixation
Nonoperative Treatment Indications • Minimal soft tissue damage • Stable fracture pattern • < 5° varus/valgus • < 10° pro/recurvatum • < 1 cm shortening • Ability to bear weight in cast or fx brace • Frequent follow-up Schmidt, et.al., ICL 52, 2003
Fracture Brace • Closed Functional Treatment 1,000 Tibial Fractures 60% Lost to F/u • All < 1.5cm shortening • Only 5% more than 8° varus • Average 3.7wks in long leg cast, then Functional fracture brace Sarmiento, JBJS 1984
Sarmiento • Union 98.5% • Time 18.1 Wks. • Short >20mm 1.4% Initial shortening = final shortening
25% patients with 25% loss of ankle-ROM Ankle Motion after tibia fractures
Natural History • Long-term angular deformities may be well tolerated without associated knee or ankle arthrosis • Kristensen F/U: 20-29 yr All patients >10 degree deformity • Merchant & Dietz F/U: 29 yrs. Outcome not associated with ang., site, immob. (37/108 patients)
Surgical Indications • High energy fracture • Moderate soft tissue injury • Unstable fracture pattern Inability to maintain reduction • Open fracture • Compartment syndrome • Ipsilateral femur fracture • Pt cannot tolerate long-leg cast Schmidt, et.al., ICL 52, 2003
Surgical Options • Intramedullary nail • ORIF with plate • External Fixation
Advantages of IM Nail • Less malunion and shortening • Earlier weight bearing • Early ankle and knee motion • Possibly cheaper than casting if time off work included Tovainen, Ann Chir Gynaecol, 2000
IM Nails – Hooper, et.al. • In a prospective study if displacement >50% angulation >10° • Nails superior to cast treatment Hooper, JBJS-B, 1991
IM Nails – Bone, et.al. Retrospective review 99 patients CastNail Time to union 26wks 18wks SF-36 74 85 Knee score 89 96 Ankle score 84 97 Bone, et.al. JBJS, 1997
Reamed vs. Nonreamed Nails • Reamings (osteogenic) • Larger Nails (& locking bolts) Hardware failure rare w/ newer nail designs • Damage to endosteal blood supply? Clinically proven safe even in open fx Forster, et.al. Injury Mar 2005 Bhandari, et.al., JOT 2000
Reamed vs. Nonreamed Nails Blachut JBJS 79A ReamedNon-Reamed # pts. 73 63 Nonunion 4% 11% Malunion 4% 3% Broken Bolts 3% 16%
IM Nails – Interlocking Bolts • Loss of alignment w/out interlocking • Spiral 7/22 • Transverse 0/27 • Metaphyseal 7/28 • Templeman CORR 1997
Infection 1-5% Union >90% Knee Pain 56% w/ kneeling 90% w/ running 56% at rest 33% Complications Court-Brown, JOT 1996
IM Nail Removal – Knee Pain • Pain resolved 27% • Marked improvement 69% • Pain worse 3% • No difference in knee pain based on tendon sparing approach Court-Brown, JOT 1996
Iaquinto, Am J. Orth 1997 63 patients reviewed Compared type of anesthesia 4.1 X greater risk of Neurologic injury w/ epidural Need to monitor exam postop Neurological Complications
Disadvantages of IM Nail • Anterior knee pain (up to 56.2%) • Risk of infection • Increased hardware failure with unreamed nails *Court-Brown et al. JOT 96
Expanded Indications • Proximal 1/3 fractures • Beware Valgus and Procurvatum • Distal 1/3 fractures • Beware Varus or valgus
Proximal Tibia Fracture • Entry site is critical • Reference is Lateral Tibial Spine
Too Low! Too Medial! Valgus Procurvatum
Semiextended Position • Neutralize quadriceps pull on proximal fragment • Medial parapatellar approach – sublux patella laterally • Use handheld awls to gently ream through the trochlear groove Tornetta, CORR Jul 1996
Hyperextended position • Pulls patella proximally to allow straight starting angle. • Universal distractor Beuhler & Duwelius, JOT 1997
Blocking (Poller) Screws • Functionally narrows IM canal • Increases strength and rigidity of fixation • 21 patients • All healed within 3-12 months • Mean alignment 1 degree valgus, procurvatum 2 degrees. Krettek C, et al. JBJS 81B: 963, 1999
Technique • Screws placed on concave side of deformity. • Proximal or distal fractures