Download
1 / 24
240 likes | 384 Vues
Ultrasound Monitoring of Fetal Growth. By Dr. Khattab KAEO Prof. & Head of Obstetrics and Gynaecology Faculty of Medicine, Al- Azhar University, Damietta. Fetal growth :

E N D
Ultrasound Monitoring of Fetal Growth By Dr. Khattab KAEO Prof. & Head of Obstetrics and GynaecologyFaculty of Medicine, Al-Azhar University, Damietta
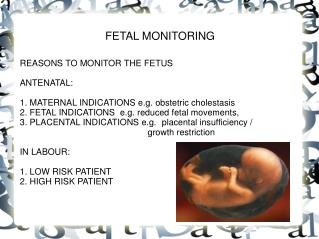
Fetal growth: Indications: Assessment of fetal growth is indicated in conditions that may be complicated with growth problems e.g. PIH, DM, PPROM, APH, previous small/large baby and small/large for date uterus.
Timing: 3rd trimester. Frequency:Every 2-4w according to clinical circumstances.
Technique: • Check gestational age from a first trimester scan. • Establish FHT and presentation. • - Trace the outer margin of the skull bone to measure the BPD & HC.
- Obtain the AC. Start with a longitudinal view of the spine, then rotate the transducer through 90 to obtain the stomach & the intrahepatic section of the umbilical vein.
The latter can not be obtained when the spine being at the 12 o'clock position. Obtaining full length of the vein means that the obtained section is too oblique. The most accurate AC is the smallest one obtained between fetal respirations. The section should be circular rather than elliptical (this can be produced by too much pressure by the transducer).
A B C D
*Hadlock model utilizing BPD, FL, HC & AC is the most accurate model. *FL, HC & AC are better to be interpreted in conjunction with the transverse cerebellar diameter measure.
B C
Low birth weight (LBW) = <2500 g infant whether born term or preterm. Small-for-date (SFD) fetuses = small for gestational age (SGA) = newborn that has a birth weight below the tenth centile for gestational age = constitutionally small fetuses and IUGR fetuses.
An IUGR fetus is the one that failed to reach its growth potential, even if still within the average birth weight centiles.
Diagnostic criteria should be based on both fetal size and placental function: * When BOTH the anomaly scan and umbilical artery waveforms are NORMAL = “normal small fetus”. * When the anomaly scan is ABNORMAL and the waveforms are NORMAL = “abnormal small fetus”. * When the anomaly scan is NORMAL and the waveforms are ABNORMAL = “FGR”.
Grades: G1 4000-4499g G2 4500-4999g G3 ≥5000g