Download
1 / 187

E N D
1. A 70-year-old right-hand–dominant male has had a tremor in his right hand for 5 years. It is now getting worse, and he is also developing a tremor in his left hand. He says his walking speed has become slower, and his wife thinks he is becoming more forgetful. There is no family history of similar problems. On examination his facial expressions seem diminished. He has a resting tremor in both hands, but it is more prominent on the right. He has a slightly stooped posture and you note a decreased arm swing when he walks. There is some resistance when his arms are passively flexed and extended at the elbows. His Mini-Mental State Examination score is 27 out of 30. Appropriate treatment at this time would include which of the following? (Mark all that are true.) • Carbidopa/levodopa (Sinemet) • Donepezil (Aricept) • Pramipexole (Mirapex) • Primidone (Mysoline) • Propranolol (Inderal)
Parkinson’s Disease Progressive neurodegenerative disorder 0.3 % of the population Cardinal signs and symptoms: Bradykinesia Resting tremor Rigidity Postural instability Item 1
Parkinson’s Disease Levodopa Carbidopa/Levodopa (Sinemet) Dopamine Agonists Pramipexole (Mirapex) Bromocriptine Pergolide Ropinirole (Requip) COMT Inhibitors-tolcapone (Tasmar) NMDA-Inhibitors-amantadine, memantine (Namenda) MAO Inhibitors Surgery Item 1b
A 75-year-old male with a history of stable angina pectoris is found to have persistently elevated blood pressure on three visits over a 2-month period. There is no evidence of renovascular hypertension on physical examination or laboratory testing. Which of the following would be appropriate at this point? (Mark all that are true.) • Evaluation for excessive alcohol use • Counseling about NSAID use • Treatment with a ß-blocker • Treatment with an ACE inhibitor • Treatment with a diuretic • Treatment with a calcium channel blocker
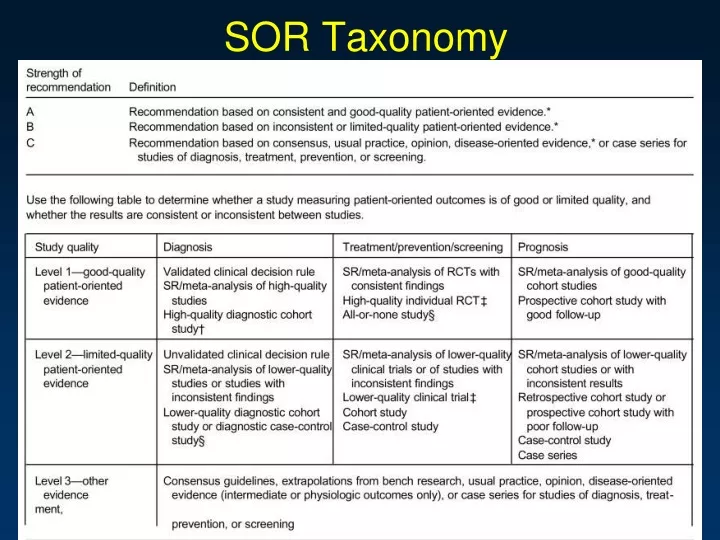
The Evidence in Hypertension in the Elderly > 2 alcoholic drinks/day increases BP in the elderly (A) Using NSAIDS increases BP in the elderly (A) Improved survival when treated with (A): B-blockers Diuretics Improved outcomes when treated with (A): ACE inhibitors ARBs Calcium Channel Blockers not first line per JNC-VII (A) Item 2
3. An 81-year-old male with New York Heart Association Class II heart failure complains of nocturia. He says he usually has to get up once during the night, and has also noticed mild hesitancy and an occasional decrease in the force of his urinary stream. He has not noted urinary frequency or dysuria, and does not feel the urge to void again shortly after urinating. He also denies hematuria. His American Urologic Association symptom score is 5. On examination there is no bladder distention, and he has a symmetrically enlarged, nontender prostate. Results of his urinalysis are normal. Which one of the following would be most appropriate at this time? A) Observation only B) A prostate-specific antigen (PSA) level C) Prostate ultrasonography D) An alpha-blocker such as tamsulosin (Flomax) E) Urologic referral
Prostate Disease Pt has life expectancy < 10 yrs so potential harm for testing for prostate cancer outweighs potential benefits (C) If symptomatic then ultrasonography Urinary retention UTI Renal failure No a-blocker as potential side effects outweigh benefits Item 3
AUASS • SYMPTOM SCORE: • 1-7 (Mild) • 8-19 (Moderate) • 20-35 (Severe)
An 82-year-old male has diabetes mellitus, heart failure, hypertension, and benign prostatic hyperplasia. His wife is 79 years old and has COPD, osteoarthritis, osteoporosis, and mild cognitive impairment. Their combined medication expenses are $5100 per year, and both are enrolled in a Medicare Part D plan. In order for them to qualify for the low-income subsidy under the federal rules for Medicare Part D, which of the following must be true? (Mark all that are true.) • Both must qualify for Medicare Part A • Both must be enrolled in a Medicare Part D plan • Both must be eligible for both Medicare and Medicaid • At least one must be disabled • Their income level must fall below 150% of the federal poverty level for a couple
Item 4a Medicare Part A • Hospital Insurance • Covers most medically necessary • Hospital care • Home health care • Hospice care
Doctor’s services Preventive care Durable medical equipment Hospital outpatient charges Lab tests Mental health care Some home health services Some ambulance services X-rays Item 4b Medicare Part BMedical Insurance
Medicare Part DLow-Income Subsidy For a married couple to qualify: Both must qualify for Medicare Part A Both must be enrolled in a Part D plan Income < 150% of federal poverty limit for a couple If eligible for Medicaid patients are automatically eligible and are not required to file an application Item 4 Item 4c
Medicare Part DLow-Income Subsidy Qualifies Patients for: $50 vs. $250 deductible 15% vs. 100% copay in coverage gap ($2,250-$5,100) Item 4 Item 4c
5. An 83-year-old female nursing-home resident with moderate Alzheimer’s disease is having increasingly frequent frightening visual hallucinations at night, despite the nursing home staff’s efforts to create a comfortable routine. Reasonable first-line nightly medications would include which of the following? (Mark all that are true.) • Buspirone (BuSpar) • Carbamazepine (Tegretol) • Lorazepam (Ativan) • Olanzapine (Zyprexa) • Risperidone (Risperdal)
Antipsychotics in Dementia First line drug choices to treat psychotic symptoms in dementia (A) Olanzapine (Zyprexa) Risperidone (Risperdal) Quetiapine (Seroquel) Buspirone (Buspar) is not recommended due to no clinical trials (C) Second line choice is carbamazepine due to side effect profile (B) Lorazepam (Ativan) is recommended only for acute agitation Item 5
6.A 73-year-old white male presents with palpable, slightly scaly areas on his face and the back of his hands. They are asymptomatic, except for being occasionally itchy. He isn’t worried about them, but his wife is. Appropriate management options include which of the following? (Mark all that are true.) • Observation only • Cryosurgery • Curettage • Topical fluorouracil (Carac, Efudex) • Topical imiquimod (Aldara) • Topical diclofenac (Solaraze)
Actinic Keratoses Can progress to SCC Cryotherapy for large number (c) Curettage for a limited number (c) Topical treatments should be considered for patients with a large number (c) 5 FU Imiquimod 5 % Diclofenac 3 % gel Chemical peels are also effective (c) Item 6
7. An 80-year-old female complains of generalized weakness and increasing difficulty carrying groceries and walking up stairs. She has been widowed for 3 years, and has been sedentary since the death of her husband. Her only medical problems are osteoarthritis and hypertension controlled with medication. She has no history of heart disease. Which of the following would be appropriate components of an exercise prescription for this patient? (Mark all that are true.) • Stress testing prior to exercise • Walking for a total of 30 minutes/day, 5 days a week • Balancing on one leg while holding on to the counter • Strength training using 1- to 2-lb weights or soup cans, performing 10 repetitions 2–3 times per week • Aquatic exercises
Exercise in the Elderly Regular exercise is associated with decrease in all cause mortality and morbidity in middle-age and older adults Modest increases in life expectancy in pts who do not begin until age 75 Should be combination of aerobic, resistance and balance/flexibility training No stress test needed to begin a moderate aerobic and resistance training program if they start slow and gradually increase activity levels (C) Item 7
Exercise in the Elderly Aerobic exercise should consist of 30 min most days of the week – 10 minute increments (A) Strength gains require effort enough to fatigue the pt after 10-15 reps per set (A) Empiric evidence suggests that balance programs improve stability and decrease risk of falls (B) Aquatic exercises limit weight-bearing, which can be helpful for patients with arthritis (A) Item 7b
8. A 78-year-old male with a previous history of hypertension and chronic atrial fibrillation has a transient ischemic attack (TIA). True statements regarding anticoagulation and antiplatelet therapy in this patient include which of the following? (Mark all that are true.) • Treatment with warfarin (Coumadin) will reduce his risk of recurrent stroke • Aspirin will be as effective as warfarin for reducing his risk of stroke • The combination of aspirin and clopidogrel (Plavix) is better than aspirin alone in reducing his risk of stroke in this patient • Aspirin should be prescribed if there is a contraindication to anticoagulation • The target INR in this patient is 2.0–3.0
Atrial Fibrillation and Anticoagulation High risk of stroke Previous TIA/stroke or embolic event HTN Poor left ventricular function Age>75 Rheumatic heart valve disease Prosthetic heart valve Item 8a
A-Fib and Anticoagulation Anticoagulation reduces stroke risk in high risk patients with AF. (A) Warfarin more effective than aspirin (not true in patients without AF) Aspirin can be used in pts who have C/I to anticoagulation but is less effective regardless of dose (A) Item 8b
A-Fib and Anticoagulation ASA + Clopidogrel insignificantly decr. risk of secondary stroke vs. ASA alone, but significant incr. in life-threatening bleeding (A) An INR < 2.0 is not effective for prevention and > 3.0 raises the risk of hemorrhage (A) Item 8c
9. You are evaluating an 80-year-old female who has a history of recurrent falls in recent months. Her medical problems include hypertension, depression, chronic atrial fibrillation, heart failure, and insomnia. Her medications include sertraline (Zoloft), alprazolam (Xanax) as needed for sleep, digoxin, lisinopril (Prinivil, Zestril), and warfarin (Coumadin). Which of her medications may be contributing to her falls? (Mark all that are true.) • Benzodiazepines • Digoxin • Lisinopril • Sertraline • Warfarin
Falls and Medications Increased risk of falls with Long and short acting benzodiazepines (A) Type 1A antiarrhythmics (B) Digoxin (B) Diuretic (B) Antidepressants No increased risk with : ACEs, CCBs, B-blockers, centrally acting antihypertensives or nitrates (B) Item 9
An 80-year-old male consults you because he has become constipated. A routine screening was negative 8 months ago. He admits that he has been less active in the last month because of pain in his knees. He also has been using an over-the-counter antihistamine for “hay fever” symptoms. Appropriate initial measures include which of the following? (Mark all that are true.) • Increased intake of fluid and dietary fiber • Increased physical activity • Bulking agents (e.g., Metamucil) • Polyethylene glycol (MiraLax) • Low-dose stimulant laxatives
Constipation in the Elderly Fluid softens stool and counterbalances the effects of medications that tend to dry the stool Fiber softens stool by adding bulk (C) physical activity gut motility (B) Bulking agents should not be used until non-medical therapy has failed (B) Item 10
Constipation in the Elderly Polyethylene glycol and stimulant laxatives can cause cramping and electrolyte disturbances so should be second line (B) Item 10b
True statements regarding cataracts include which of the following? (Mark all that are true.) • Family physicians should perform fundoscopy, visual acuity testing, and pinhole testing on all patients suspected of having cataracts • Referral to an ophthalmologist is not necessary for patients with suspected cataracts if their visual acuity is 20/40 or better • Otherwise healthy older adult patients scheduled for cataract surgery under local anesthesia do not require routine preoperative medical evaluation • Outpatient surgery is recommended for cataract extraction
Cataracts Testing on patients with suspected cataracts (B) Fundoscopy Visual acuity Pinhole testing Ophthalmology referral to test for glare sensitivity No need for surgical clearance as local anesthesia carries minimal risk (A) No benefit to inpatient stay (B) Item 11
12. A 78-year-old female presents with diffuse abdominal pain, abdominal distention, diminished bowel sounds, and nausea with occasional vomiting. Her medical history includes type 2 diabetes mellitus, and well-controlled hypertension. She has a previous history of right upper-quadrant colicky pain, but no history of previous abdominal surgery. A CBC reveals a hematocrit of 38.0% (N 36.0–46.0) and a WBC count of 11,000/mm3 (N 4300–10,800). Serum electrolytes, amylase, and lipase are within normal limits. A urinalysis is normal. Plain films of the abdomen show small bowel obstruction, air in the biliary tract, and a calculus. The most likely diagnosis is A) diverticulitis B) acute cholecystitis C) gallstone ileus D) acute pancreatitis
Abdominal Pain Gallstone ileus Abdominal film classically shows SBO Air in biliary tract Calculus Item 12
Abdominal Pain Diverticulitis Pain more localized and not associated with calculus disease or air in biliary tract Acute Cholecystitis No air in biliary tract, pain is more commonly R sided Acute Pancreatitis Pain radiates to the back and associated with elevated Amylase and lipase Item 12b
13. An 84-year-old male with Parkinson’s disease lives at home with his wife. At a routine follow-up visit she tells you that she is concerned because he likes to walk around inside the house but has fallen twice in the past 3 months. Which gait assistive device should you recommend? A) A standard four-point walker B) A two-wheel walker C) A four-wheel walker D) A wheelchair
Gait Assistive Devices 4-wheel walker easier to initiate than a standard 4-point or 2 wheel walker for Parkinson’s patient. (C) Less likely to fall backward than with a 4-point walker (C) Wheelchair too restrictive at this point. Item 13
14. Consequences of polypharmacy in elderly patients can include which of the following? (Mark all that are true.) • Medication nonadherence • Adverse drug events • Age-related impairment of the immune system • Drug-drug interactions • Drug-disease interactions
Polypharmacy in the Elderly Elderly at increased risk for complications due to: Underlying diseases Physiologic changes due to aging Poor physical and cognitive health Increased potential for Drug-drug interactions Drug-disease interactions Adverse drug events Non-adherence Item 14
15. An 87-year-old female has a 20-year history of type 2 diabetes mellitus. Her current medications include metformin (Glucophage), lisinopril (Prinivil, Zestril), and aspirin. True statements regarding the care of this patient include which of the following? (Mark all that are true.) • Because of her age, her blood pressure targets are higher than those for younger patients with diabetes. • Quarterly hemoglobin A1C levels are indicated. • An LDL-cholesterol level of 140 mg/dL would suggest the need for intervention. • Aspirin is no longer indicated because of the patient’s age.
Diabetes in the Elderly Blood pressure goals are the same for all ages – 130/80 (B) No evidence that quarterly HgbA1C measurements benefit - should tailor evaluations. (C) If LDL > 130 lifestyle intervention or medication is indicated (B) ASA is still important for this pt. (B) Item 15
16. An 85-year-old female with Alzheimer’s disease of moderate severity lives alone. She is having increasing difficulty caring for herself, and her family is concerned about her safety. The family is considering care options and asks for your opinion. The patient has repeatedly stated that she wishes to remain in her home and refuses assistance other than family. When counseling the patient and family regarding appropriate placement, factors to consider include which of the following? (Mark all that are true.) • The level and type of care required • Patient and family finances • The patient’s ability to participate in decisions • The progression rate of the Alzheimer’s disease • The amount and type of help that family can provide
Elder Care Assistance Pts with moderate Alz often require 24 hr supervision due to safety concerns This can be provided At home Assisted living Nursing homes Goal: Optimize quality of life while providing required assistance. Item 16
Elder Care Assistance When choosing options it is important to consider: The patient’s physical and cognitive health – need for assistance with ADLs or decisions Overall medical condition Need for rehabilitation services Need for skilled nursing services Level of supervision required Patient and family finances and insurance coverage Life expectancy Item 16a
17. A 72-year-old male with multiple myeloma presents with worsening pain in the back and ribs. He has tried both ibuprofen and acetaminophen with codeine, but neither has provided adequate pain relief. Which one of the following would be the best agent for pain control? • Amitriptyline • Meperidine (Demerol) • Morphine • Propoxyphene (Darvon)
Pain Management Item 17 Morphine is the gold standard for controlling cancer pain (A) Amitriptyline can cause orthostatic hypotension and anticholinergic SE so not recommended (A)
Pain Management Item 17b Meperidine has risk of delirium and seizures (B) Propoxyphene associated with hip fx and provides no better analgesia than acetaminophen or other analgesics with better safety profiles (B)
An 85-year-old retired college professor has had an acute stroke. True statements regarding management of possible depression following his stroke include which of the following? (Mark all that are true.) • He should be screened for anxiety and depression within the first month after the stroke • Treatment of mood disorders should focus on a single disorder to avoid complicated treatment regimens • He should be placed on antidepressants prophylactically • If he has a persistent depressed mood > 6 weeks after the stroke, he should be offered antidepressant medication • If he has severe, persistent, or troublesome emotionalism, he should be offered antidepressant medication