Download
1 / 18
190 likes | 464 Vues
Schistosomiasis Vanessa De Danzine , MPH student Walden University. PH 6165-4 Dr. Raymond Thron Spring 2009. Who is Theodor M. Bilharz?. Theodor Maximilian Bilharz (1825-1862) was a German physician and parasitologist who discovered Schistosomiasis in Egypt in 1851. Schistosomiasis.

E N D
SchistosomiasisVanessa De Danzine, MPH studentWalden University PH6165-4 Dr. Raymond Thron Spring 2009
Who is Theodor M. Bilharz? Theodor Maximilian Bilharz (1825-1862) was a German physician and parasitologist who discovered Schistosomiasis in Egypt in 1851.
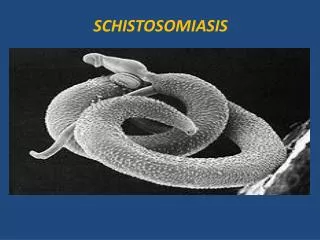
Schistosomiasis Schistosomiasis is also known as bilharzia, bilharziasis or snail fever. It is a parasitic disease in humans caused by one of the species of fluke of the genus Schistosoma.
Life Cycle of the Schistosomes Schistosomes have a complex life cycle. The head of the cercaria transforms into an endoparasitic larva, the schistosule which passes several days in the skin after penetration, then enters the venous circulation system then migrates to the lungs (5-7 days). After 15 days of travelling through the circulatory system to the hepatoportal circulation they mature into adults and mate.
Where in the body do they migrate? • The schistosomes harbor in many orifices of the body. Depending on the specie, the schistosomes can migrate to the intestines, liver, abdomen, bladder and lungs where they attach to the walls of the lumen and reproduce.
Prevalent Areas Schistosomiasis is most prevalent in developing countries in Africa, South America, the Caribbean, the Middle East and Asia.
Mortality/Morbidity • It’s low mortality rate can cause extensive internal organ damage. Impairment of growth and development are prevalent in children. • Mortality rates as high as 25% are often presented in Acute Schistosomiasis (CDC, 2005). • Although Chronic Schistosomiasis can often be asymptomatic, significant morbidity can be presented with end stage hepatosplenic disease with portal hypertension and cur pulmonale.
Severity of Schistosomiasis SEX AGE The highest peak of infection are in children and adolescents ages 10-19 years. Cognitive behavior, physical fitness, fatigue and poor school age performance are also affected. • One particular specie of schistosomiasis that causes genital lesions in 30% of women who are infected is the Schistosoma haematobium (Behrman, 2008). • Women with vulval lesions may be at a greater risk for HIV transmission (Behrman, 2008).
How is Schistosomiasis Transmitted? Schistosomiasis can be transmitted in one of two ways: It’s most common denominator is via snails who harbor in freshwater. Cercariae (lavarae) is released daily from the snail. The cercariae is very mobile in turbulent water where it becomes attracted to the chemicals found on the human skin.
How is Schistosomiasis Transmitted? (cont.) Via humans - Once the water becomes contaminated with Schistosoma eggs it penetrates the human skin where they are often found to be swimming, bathing or washing. Enzymes are secreted to break down the human skin protein which thus allows penetration of the cercaria head. Human then urinate and/or defecate in these freshwaters releasing infected eggs therefore increasing the transmission rate of Schistosomiasis.
Signs and Symptoms The most common signs and symptoms are often indicative of common illnesses and disease and often overlooked. Fever, bloody diarrhea, abdominal pain, headache, malaise and cough can be related to a few differential diagnosis of gastroenteritis, inflammatory disease or Salmonella infections.
Signs and Symptoms (cont.) The addition of eosinophila and hepatosplenomegaly can be uniquely identified with Schistosomiasis.
Acute Schistosomiasis Dermatological manifestation of maculopapular skin lesions can appear after immediate contact with the cercariae.
Chronic Schistosomiasis This advance stage of schistosomiasis can yield hepatic disease. In the presence of hepatitis B or hepatitis C, increase hepatic dysfunction can occur. This dysfunction can further progress to hepatocellular carcinoma.
Prevention • Since most developing countries do not have proper drainage and sewage systems of their water usage, personal hygiene and domestic use should be limited. • Individuals can avoid swimming or bathing in freshwater contaminated with schistosomiasis. • Drinking water should be boiled for at least 1 minute.
Treatment • Antihelminthic therapy is the treatment of choice. • Praziquantel (Biltricide) is widely used. • This drug is classified as Class B – for pregnant women. Fetal risk has not been confirmed in human studies, only in some animal studies. It is contraindicated. • Different doses are indicative for specific species.
Recovery Period • After extensive periods of antihelmintics treatment result in 60-98% (WHO, 2009) cure rate, thus decreasing morbidity and restoring confidence of long term disability. • Decrease blood and iron loss which have impaired cognitive behavior and affect school age children can be repleminished with iron supplements. • Renal failure can be rectified with treatment of urinary schistosomiasis as early as 6 months. • Hepatic disease may show significant improvements within months to years post treatment. • Intestinal recovery is immediately soon after treatment.
References • Centers for Disease Control and Prevention (CDC). (2005). Retrieved on April 16, 2009 from www.cdc.gov. • Behrman, A.J. (2008). Schistosomiasis. Emergency Medicine: Infectious Diseases. Retrieved on April 19, 2009 from www.emedicine.medscape.com. • World Health Organization (WHO). (2009). Retrieved on April 22, 2009 from www.who.int. • Photos compliment of Google imagine gallery. Retrieved on April 16, 2009 from www.google.com.




![[Aaron Akindiya] Walden University](https://cdn5.slideserve.com/9327563/slide1-dt.jpg)