Download
1 / 35
400 likes | 634 Vues
Cell Based Model. Galila Zaher, MRCPath Assistant Professor Consultant Hematologist KAUH. HEMOSTASIS. TF. VIIa. INITIATION OF HEMOSTASIS. TF-BEARING CELL. PROPAGATION OF HEMOSTASIS. ACTIVATED PLATELET. THROMBIN. FIBRIN HEMOSTATIC PLUG. II. X. VIII/vWF. VIIIa. V. Va. VIIa.

E N D
Cell Based Model Galila Zaher, MRCPath Assistant Professor Consultant Hematologist KAUH
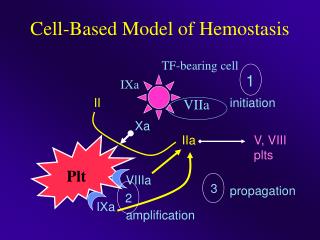
HEMOSTASIS TF VIIa INITIATION OF HEMOSTASIS TF-BEARINGCELL PROPAGATION OF HEMOSTASIS ACTIVATED PLATELET THROMBIN FIBRIN HEMOSTATIC PLUG
II X VIII/vWF VIIIa V Va VIIa Xa Va TF IIa TF-bearing cell XI XIa IX VIIa TF IXa II platelet X VIIIa IIa Xa Va IXa XIa activated platelet IX Normal Hemostasis
Thrombin FV FVIII IIa (THROMBIN) FVa FVIIa FIBRINOGEN FIBRIN (SOLUBLE FIBRIN MONOMERS) FXIIIa STABILIZED, CROSS-LINKED FIBRIN (HEMOSTATIC PLUG) FIBRINOLYSIS TAFI
Fibrin Structure Thrombin: 0.60 U/mL (a) (b) 0.10 U/mL (c) 0.05 U/mL (d) 0.03 U/mL Blomback et al. 1994
Thrombin Activity 0.05 With FVIII present 0.045 (- FXI) 0.04 FVIII-deficiency 0.035 + 50 nM FVIIa 0.03 Thrombin activity (dA405/min) 0.025 + 150 nM FVIIa 0.02 0.015 0.01 0.005 0 0 20 40 60 80 100 120 140 Time (min) Kjalke et al. 1999
FACILITATE HEMOSTASIS • Enhance thrombin generation • Inhibit fibrinolysis • WHY FVIIa? • FVIIa not enzymatically active unless in complex with TF • FVIIa not immediately inhibited by AT • FVII present in plasma • FVIIa added to hemophilia plasma with inhibitors normalized APTT
Potential Use of rFVIIa • Increases thrombin generation • Hemophilia (FVIII/FIX deficiency) • Platelet disorders • Diffuse bleeding triggered by surgery and trauma • Impaired initial hemostasis • FVII-deficiency • Liver disease (low levels of FVII) • OAC therapy (low levels of FVII)
Hemophilia II VIII/vWF VIIIa X V Va Xa VIIa Va TF IIa XI XIa TF-bearing cell VIIa TF platelet II X IIa VIIa Va Xa activated platelet
Haemophilia • FDA-approved Hemophilia with inhibitors • Efficacy in major surgery 90-100% (90-100 µg/kg q2 for first 48 hs, q4 hours on D3-D4then to q6 hours for another week (Shapiro et al 1998; Ingerslev et al 1997) • Efficacy in serious bleedings 83-95% (Lusher et al 1998) • Efficacy in home treatment 92% (Key et al 1998) • Acute bleeds in hemophilia >5 BU • No good laboratory markers for monitoring efficacy • TEG or Trend of quantitative D-dimer levels as a blood counts and fibrinogen level
COST-EFFECTIVENESS in mild-mod HA bleeding – UK study Clinical effectiveness – • rFVIIa: mean 2.3 doses of 90 ug/kg controlled 92% of all minor bleeds within 24 hrs (Key et al 1998). • FEIBA (aPCC): mena 3 doses of 75 units/kg controlled 79% of minor bleeds within 36 hrs (Hilgartner)
COST EVALUATION MILD-MOD BLEEDINGS IN HAEMOPHILIA rFVIIa is safe and has a higher efficacy relative to other treatment options”.
The FENOC study • FEIBA (activated prothrombin complex concentrate (aPCC). • Test equivalence of products in treatment of ankle, knee, and elbow joint bleeding. • A prospective, open-label, randomized,crossover • Data for 96 bleeding episodes contributed by 48 participants were analyzed. • FEIBA and NovoSeven appear to exhibit a similar effect on joint bleeds, although the efficacy between products is rated differently by a substantial proportion of patients. 2007 ASH
FVII-DEFICIENCY • Autosomal recessive 1/500 000 persons • Genetic & clinical heterogeneity • FVII activity <1% severe • Prolonged PT; normal APTT • There is only small number of patients available (case series) • FDA-approved dose 15 -30µ g per kg, q6 -12 hs • Monitored by PT & its correction correlate well with achievement of clinical hemostasis
USE OF rFVIIa IN FVII-DEFICIENCY • N=32 treated in Compassionate and ER between 1988- 1999. • Treated at 28 sites in 6 countries (AUS, DK, I,Malaysia, USA) • Non-surgical episodes: 43 joint bleeds • EFFECTIVE in 37/43 (86%) episodes independent on location of bleed. • Surgical episodes: 26 • EFFECTIVE in 25/26 (96%) episodes. • 10 adverse events 2 pt developed Abs against FVII • FDA-approved dose 15 to 30µ g per kg q 6-12 hours • Monitored by the PT.
Preliminary guidelines for off-label use proposed in 2004 • The consensus panel related use of rFVIIa as appropriate in : • Cardiac, thoracic, aortic, and spinal surgery • Hepatic resection • Hysterectomy; postpartum bleeding • Severe, multiple trauma substantial blood replacement ineffective. • Non traumatic ICH <4 hours since onset of symptoms • Anti-coagulated patients with expanding hematomas. • Doses of 41 to 90 µg / kg recommended in adults for all scenarios. • Correction of the pH value >7.2 • Multitrauma patients is 100 - 140 µg/ kg repeat dose
European Recommendations on the use of rFVIIa as an adjunctive treatment for massive bleeding –
Trauma. • Uncontrolled massive hemorrhage is 2nd cause of death • Massive hemorrhage : surgical / vascular and a coagulopathic component. • ‘Lethal triad‘: consumption , dilution and metabolic disorders • In cases of injury, TF is brought into contact with naturally occurring FVIIa, to initiate thrombin • Pharmacological doses, rFVIIa bind activated platelets at the site of injury and activate FIX and X directly, leading to a thrombin burst
BluntTrauma • Successful report for trauma in an Israeli soldier • Case series of 36 patients stopped bleeding in 72% of cases • Several case studies ,case series , retrospective cohort • Conventional hemostatic measures have failed. • Promising addition to thrapeutic armamentarium • Multicenter, randomized, double-blind, placebo controlled study by Boffard • Initial dose of 200 µg/kg , then 100 µg/kg, at 1 and 3 hours • Produced a significant reduction in the primary endpoint RBC transfusion requirements , need for massive transfusion, and incidence of respiratory failure Grade B • Penetrating trauma are uncertain, no recommendations can be made for this indication. Grade B
Penetrating Boffard et al.: J Trauma 2005
Recommendations on the use of rFVIIa as an adjunctive treatment for massive bleeding – a European perspective • Not be used in prophylactically in elective surgery (grade A) • Use of rFVIIa in blunt trauma (grade B). • Not be recommended for use in penetrating trauma (grade B) • Not be recommended for use in liver surgery (grade B) • Not be recommended for use in or in bleeding episodes in patients with Child–Pugh A cirrhosis (grade B). Bleeding after cardiac surgery (grade D). • Postpartum hemorrhage (grade E) • Uncontrolled bleeding in surgical patients (grade E) • Monitoring of rFVIIa efficacy should be performed visually and by assessment of transfusion requirements (grade E), • Critical Care 2006, 10:R120
Warfarin Reversal • Dramatic increase in number of patients receiving OAC • Interindividual variation (environmental and genetic) • Incidence of fatal haemorrhage :1%/Y. • Increased risk of ICH > 50 y compared with non-anticoagulated 10x • Reversal :seriousness of bleeding , thrombotic risk and speed and completeness of reversal • Options : dose omission ,vit K & factors replacement • FFP or PCCs
Warfarin ReversalPCCs • Intermediate purity plasma products • Only HTDEFIX is licensed in UK for warfarin reversal • PCCs, (‘‘4 factor concentrates’’), OR low VII (3 ) • Amounts of protein C and S • Optimum dose not established. • Thrombogenicity, exacerbation of DIC are dose related • Current cost in UK (single treatment for a 70 kg individual £437 -£875). • More expensive > FFP. ( unit of produced from UK plasma costs about £30). • FFP that is methylene blue treated or produced from non-UK plasma is more expensive.)
Warfarin Reversal rFVIIa • Advocated in the management of bleeding • Studied in a small number of studies • Normalises the INR in anticoagulated • Dose range, 15–90 mg/kg • Small numbers of patients with ICH successfully treated with rFVIIa have been reported recently.54–56 • Lin J, J Neurosurg 2003;98:737–40. • Sorensen B, Blood Coagul Fibrinolysis 2003;14:469–77 • On the basis of this limited data, the role of rFVIIa in warfarin reversal remains unclear.
Use in intracranial hemorrhage. • A recent report in ICH in adults • Control the expansion of intracranial hematomas in elderly patients, improving neurologic outcome and significantly decreasing mortality. • Serious thromboembolic events were higher in the treated groups (7% vs. 2% for placebo). • Bijsterveld NR, Circulation 2002;106:2550-4.
SAFETY PROFILE • Theoretical increased risk of thrombotic events • rFVIIa bind to active PLTs , hemostatic activity should be restricted to vessel injury (TF is exposed & PLTs are locally activated) • Experimental evidence for localized effect in rabbit model • Dec 1995 -Jan 2005,total amount of rFVIIa released 680,245 standard doses :approved or “off-label” use, • Over this postmarketing period, 123 thrombotic corresponding to a mean of 1/10000 thrombotic • Review in patients with acquired and congenital hemophilia with inhibitors, incidence of thrombotic events was low
SAFETY PROFILE • Review of 13 controlled clinical trials, 1178 patients with coagulopathy No significant association was found between exposure to rFVIIa and incidence of thrombotic events????. • No inhibitors reported neither in HA nor off-label use. • Two patients with FVII-DEFICIENCY (no FVII protein) developed transient inhibitors against FVII. • Thrombotic complication: elderly with existing atherosclerotic disease. • FDA report :Arterial and venous thromboembolic events .Half occurred in first 24 hours after last rFVIIa dose. • Underlying medical conditions existed in some. • Lack sufficient information dosage ,concomitant medications, pre-existing medical conditions and the confounding indication;
Advantages Disadvantages Advantages • Rapid onset of action • Low-volume dosing • Recombinant nature alleviating infectious disease transmission • Low risk of thrombogenicity :increasing cases being reported of thromboembolic manifestations Disadvantages • Substantial cost $1000 per milligram • Risk of thrombosis • Variability of current recommended dose and dosing intervals • Short half-life • Limited data pertaining to safety and efficacy, • Problems with monitoring its efficacy.
SUMMARY • Great potential in achieving hemostasis in patients refractory to traditional treatments. • Significant cost and uncertain benefit in many clinical situations, it should not be used indiscriminately. • Transfusion service , pharmacy OR content expert in hemostasis are appropriate gatekeepers • The ordering physician must demonstrate to a gatekeeper that the patient meets established criteria • For off-label use a maximum of two doses • Further doses given only after additional expert consultation. • FDA-approved indication :Hemophilia patients with inhibitors & Congenital FVII deficiency
Hemostatic Defects Most common are: • Low platelet counts • Low levels of vit K-depandent coagulation factors (FVII, FX, FIX, FII, ProtC) • lowered fibrinogen • lowered FVIII and FV - increased fibrinolysis
Use in qualitative PLT disorders. • Ability of pharmacologic doses to enhance rate of thrombin generation on activated PLTs • Midlevel evidence and case reports exist. • Glanzmann’s thrombasthenia :reports with good results. • A report of 33 episodes in 7children 60% excellent response if treated within 12 hours of onset of bleeding. • Surgical prophylaxis and excessive menstrual bleeding • Doses of 90 to 120µ g per kg • Approved for use in Europe • Poon MC, international survey. J Thromb Haemost 2004;2:1096-103.