Download
1 / 70
700 likes | 922 Vues
Dr .Patibandla Sowjanya Dept. Accident & Emergency Medicine Vinakaya Mission Research Foundation (D.U) Salem, Tamilnadu, India. Trauma in Pregnancy & Paediatric Trauma. Two for One Caring for the Pregnant Trauma Patient. Incidence. The Leading cause of non-obstetrical mortality

E N D
Dr .Patibandla Sowjanya Dept. Accident & Emergency Medicine Vinakaya Mission Research Foundation (D.U) Salem, Tamilnadu, India. Trauma in Pregnancy & Paediatric Trauma
Incidence • The Leading cause of non-obstetrical mortality • Causes of Trauma (1) • Motor vehicle accident • Domestic abuse & assault • Falls • Penetrating injury (1)Connolly A, Katz VL, Bash KL, et al: Trauma and pregnancy. Am J Perinatol 14:331-336, 1997
Cardiovascular • Some alterations mimic shock supine hypotensive syndrome • Some alterations hide shock Increased blood volume • Some alterations can aggravate traumatic bleeding uterus
Supine Hypotensive Syndrome (1) Milson I, Forssman L: Factors influencing aortocaval compressionin late pregnancy, Am J Obtst Gynecol 148: 764-771, 1984
Respiratory system • Respiratory alkalosis • Reduce oxygen reserve • Residual volume decreased by 40% • Respiratory rate increased • Impaired buffering capacity • Diaphragm elevation
Gastrointestinal system • Decrease GI motility • Decrease peritoneal irritation • Upward position of abdominal viscera
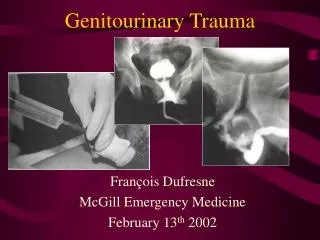
Genitourinary System • Bladder is displaced upward >10 wks • Dilatation of renal pelvis and ureters
Injuries unique to pregnancy • Premature Contractions • Rarely progress to preterm delivery • Tocolysis is not proven in trauma.(1) (1) GoodwinTM, Breen MT: Pregnancy outcome and fetomaternal hemorrhage after noncatastrophic trauma, Am J Obstet Gynecol162: 665-671, 1990.
Abruptio Placenta • Different elastic properties in uterus & placenta “shearing” • 3 % of minor trauma and up to 50 % in severe trauma
Uterine Rupture • Rare, 0.6 % of severe abdominal trauma (1) • Direct trauma after 12 wks of gestation • Prior Surgery (C/S ) the risk 1. Pearlman MD, Tintinalli JE, Lorenz RP: Blunt trauma during pregnancy, N Engl J Med 323:1609, 1990
Maternal-Fetal hemorrhage • 4 to 5 X more common in injured pregnant women • Causes isoimmunization & fetal death • ? Kleihauer-Betke test - volume of fetal blood • To determine amount of Rhogam needed
Penetrating Injury • Gravid uterus alter injury pattern to the mother. • If missile enter upper abdomen; increased probability of harm • If enters below uterine fundus visceral injury less likely (1) Awwad JT et al: High-velocity penetrating wounds of the gravid uterus: Review of 16 years of civil war, Obstet Gynecol 83:259, 1994.
Pregnancy Test • Every women in the Reproductive age group must be tested for pregnancy
Modalities for Evaluating Trauma • Plain x-rays • Ultrasound • CT & MRI • Cardiotocographic Monitoring • DPL • Laparotomy
Ultrasound • Best modality to assess both fetus and mother • Not sensitive: • Colonic lesions • Sub-placental hematoma • Safe procedure
Fetal Monitoring • If < 24 weeks, intermittent fetal doppler • If > 24 weeks, then continuous cardiotocographic monitoring to assess FHR and uterine activity
A 28 yrs female with 29 weeks pregnancy brought to ER after RTA with the suspected abdominal injury . HR – 110, BP – 110 / 70, Spo2 – 98% on RA , RR – 28/min , GCS – 15/15 C/O – diffuse pain in chest & abdomen
Remember • A Normal ABG Report in a Pregnant Patient Is ABNORMAL
Management • Avoid distractions and avoid focus on the fetus. • Be aggressive! But temper with common sense. • An apparently stable mother may be compensating at expense of the fetus.
Pre-hospital Consideration • Prevention of maternal hypoxia and hypotension. • Airway patency with adequate O2. • Left lateral tilt. • Volume replacement.
Initial maternal Resuscitation Airway Assess & control Pre oxygenate and sellick’s maneuver Breathing Assess and manage Circulation Assess maternal circulation IV access Tilt to left if > 20 wks
Key interventions to Prevent Arrest Place the patient in the left lateral position or manually and gently displace the uterus to the left. Give 100% oxygen. Give a fluid bolus. Immediately reevaluate.
Modification to BLS Guidelines for Arrest • Relieve aortocaval compression by manually displacing the gravid uterus. • Generally perform chest compression higher on the sternum to adjust for the shifting of pelvic and abdominal contents toward the head.
Perimortem Cesarean Section • ~200 successful cases reported in the literature • Maternal CPR <5 minutes, fetal survival excellent • 23 weeks gestation survival chance is 0% • Maternal CPR >20 minutes, fetal survival unlikely
Perimortem Cesarean Section • 4 Minute Rule: Maternal CPR for 4minutes, Infant should be delivered by the 5th minute.
Perimortem Cesarean Section • Vertical incision from xyphoid to pubis • Continue straight down through abdominal wall and peritoneum • Cut through uterus and placenta • Bluntly open uterus and remove fetus • Cut and clamp cord
Remember • Anatomic and physiologic changes • Vigorous fluid and blood replacement • Treat the mother first and treat her just like any other trauma patient
When to Intervene and Consult • EARLY !
Remember What is Best for the Mother is Best for the Fetus!
Unique characteristics • Size & shape : smaller body mass-greater force applied per unit body area • Skeleton: more pliable – internal organ damage -without overlying bony # • Equipment : appropriate size
Airway • Smaller in diameter,shorter in length • Epiglottis – long, floppy,narrow • Large occiput-flexion • Narrowest portion –below vocal cords • Larynx – Anterior & caudal • Large tongue
Airway management • Oxygenation • Oral airway • Intubation