Download
1 / 5
50 likes | 250 Vues
Varón de 44 años con disnea, pausas de apnea, broncorrea de aprox. 1 mes evolución. CASO CLÍNICO. HOSPITAL UNIVERSITARIO DE GETAFE. Madrid Karina Rodríguez (1) , Pierina Rubio (2) , Juliana Rodríguez (2) , Joaquín Costa (3).

E N D
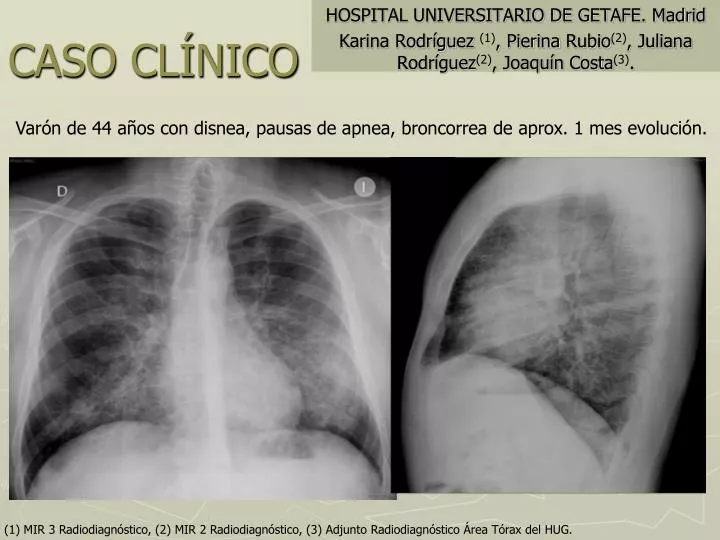
Varón de 44 años con disnea, pausas de apnea, broncorrea de aprox. 1 mes evolución. CASO CLÍNICO HOSPITAL UNIVERSITARIO DE GETAFE. Madrid Karina Rodríguez (1), Pierina Rubio(2), Juliana Rodríguez(2), Joaquín Costa(3). (1) MIR 3 Radiodiagnóstico, (2) MIR 2 Radiodiagnóstico, (3) Adjunto Radiodiagnóstico Área Tórax del HUG.
1. ¿Cómo describirías la afectación visualizada en las imágenes (TC)? A) Nódulos con halo en vidrio deslustrado. B) Engrosamiento peribronquial con “árbol en brote”. C) Enfisema centrolobulillar con panalización. D) Vidrio deslustrado y engrosamiento del intersticio interlobulillar. 2. ¿ Cuál de las siguientes entidades cursa con un patrón “crazypaving” o empedrado? A) Fibrosis pulmonar idiopática. B) Proteinosis alveolar. C) Histoplasmosis. D) Tuberculosis. PREGUNTAS
CONCLUSIÓN • Diagnóstico: Biopsia y lavado bronquioloalveolar mostró abundante material proteináceo y cuerpos redondos acelulares PAS-diastasa positivo. Inflamación predominantemente linfocítica. HALLAZGOS COMPATIBLES CON PROTEINOSIS ALVEOLAR. • Enfermedad caracterizada por alteración en la homeostasis de surfactante con depósito alveolar de material lipoproteináceo, mayoritariamente idiopática. • Síntomas insidiosos (resfriado, fiebre y moderada disnea) ♂:♀ = 4:1, tendencia a sobreinfección por Nocardia en los no tratados. 30% asintomáticos. • Tratamiento es el lavado broncoalveolar, mayoría mejora tras un ciclo, algunos requieren varios. Algunos pacientes recurren. • Evolución: mejoría tras el primer curso de lavado broncoalveolar.
BIBLIOGRAFÍA • Aletta Ann Frazier, MD • Teri J. Franks, MD et al. From the Archives of the AFIP: Alveolar proteinosis. RadioGraphics 2008; 28:883–899. • Chang Hyun Lee,MD. The crazy-paving sign. Radiology 2007; 243:905–906. • J. Michael Holbert ,Philip Costello, Wei Li, et al. CT Features of Pulmonary Alveolar Proteinosis. AJR 2001;176:1287–1294 • Santiago E. Rossi, MD. Jeremy J. “Crazy Paving” pattern at thin-section CT of the Lung: Radiologic-Pathologic Review. RadioGraphics 2003; 23:1509–1519. • Janet E. Kuhlman, MD. Pneumocystic Infections: The Radiologist’s Perspective’. Radiology 1996; 198:623-635. • W. Richard Webb,MD. Thin-Section CT of the Secondary Pulmonary Lobule. Radiology 2006; 239:322-338. • W. Richard Webb. Enfermedad pulmonar difusa asociada a lípidos. Radiología pulmonar y cardiovascular. Edición en español. Madrid: Marbán; 2009. p.498-502. • Kumar. Robbins and Cotran Pathologic Basis of Disease. Professional Edition, 8ª ed. Saunders:2009. Chapter 15.