Download
1 / 6
60 likes | 148 Vues
Respiration. Functions of upper respiratory system. Functional Anatomy. Pulmonary volumes and capacities. Muscles of respiration. Pulmonary and alveolar ventilation. Warming up of air (within body temperature)

E N D
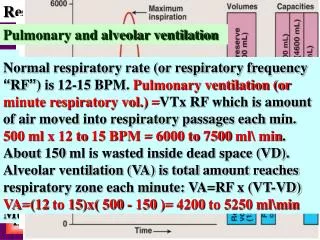
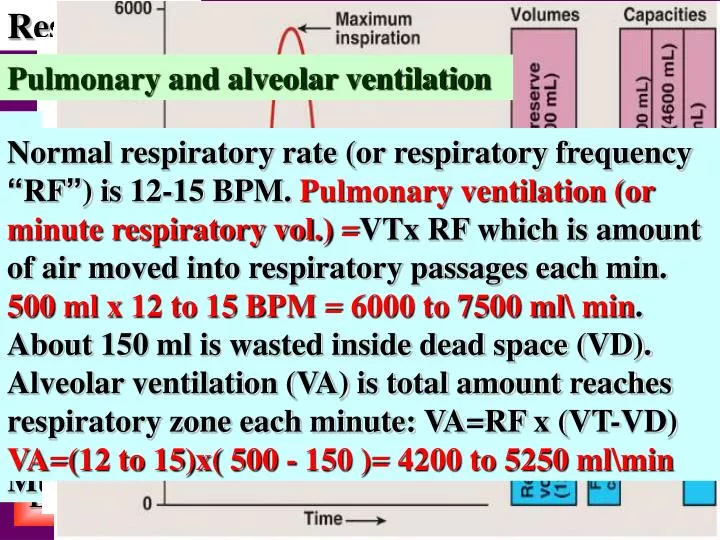
Respiration Functions of upper respiratory system Functional Anatomy Pulmonary volumes and capacities Muscles of respiration Pulmonary and alveolar ventilation Warming up of air (within body temperature) Humidification of air (about fully saturated with water vapor, otherwise, lung crusting & infection). Filtration of large foreign particles: Nostrils' hair Turbulent precipitation: Particles larger than 6μ in diameter on mucous coat of nose & nasopharynx. Gravitational precipitation : Smaller than 6μ dia. particles within bronchioles, taken up by alveolar macrophages or exhaled out. Mucous coat & cilia, move to cough or swallow Normal quiet breathing: Contraction & relaxation of diaphragm, changes vertical dimension of chest. Inspiration (inhalation): Active, negative pressure, syringe-like manner. Expiration (exhalation): Passive, relaxation of dia-phragm & elastic recoil of lung, thoracic & abdom-inal tissues, raises pressure Pulmonary volumes are: 1-Tidal volume (VT): Volume inspired & expired each quiet breath. It is about 500 ml. 2-Inspiratory reserve volume (IRV): Maximum volume can be inspired above VT. About 3000 ml. 3-Expiratory reserve volume (ERV): Maximum amount expired after VT. About 1100 ml. 4-Residual volume (RV): Volume remaining after the most forceful expiration. About 1200 ml. Normal respiratory rate (or respiratory frequency “RF”) is 12-15 BPM. Pulmonary ventilation (or minute respiratory vol.)=VTx RF which is amount of air moved into respiratory passages each min. 500 ml x 12 to 15 BPM = 6000 to 7500 ml\ min. About 150 ml is wasted inside dead space (VD). Alveolar ventilation (VA) is total amount reaches respiratory zone each minute: VA=RF x (VT-VD) VA=(12 to 15)x( 500 - 150 )= 4200 to 5250 ml\min All these volumes & capacities are in average sized healthy young males but, they are about 20%-25% less in females. They are also lower in older, shorter, asthenic, black complexion, lowlander and smoker subjects than in younger, taller, athletic, white complexion, highlander and non-smoker subjects respectively Intrathoracic part involves lower part of trachea, carina, two main bronchi (primary bronchi), other bronchial tree (about 34 generations): Lobar bronchi (secondary bronchi), lobular or segmental bronchi (tertiary bronchi), terminal bronchioles, respiratory bronchioles, alveolar ducts, atria, alveolar sacs and alveoli. The main function of respiratory system is to take in O2 & give out CO2. It also regulates acid-base balance & heat & participates in phonation & vocalization. Respiratory system is divided into extrathoracic & intrathoracic parts: Extrathoracic part: Nose, nasopharynx (& mouth & oropharynx), larynx and upper part of trachea Functionally, the respiratory system is divided into two main zones: Conductive zone: no gas exchange, transmits air to next zone, anatomical dead space, from nose to terminal bronchioles & respiratory zone: gas exchange, involves transitional zone, from respiratory bronchioles to alveoli. Respiratory membrane: 6 µ in diameter, surface area 140 m2 , six layers: 1. Alveolar fluid lining alveoli (with surfactant) 2. Single layer of squamous alveolar epithelium 3. Basement membrane of alveolar epithelium 4. Narrow interstitial space 5. Basement membrane of capillary endothelium 6. Single layer of squamous capillary endothelium Pulmonary capacities are: 1-Inspiratory capacity (IC)= VT + IRV ≈ 3500 ml. 2-Functional residual capacity (FRC) FRC = ERV + RV ≈ 2300 ml. 3-Vital capacity (VC) = VT+ IRV+ERV ≈ 4600 ml. 4-Total lung capacity (TLC) = VC + RV ≈ 5800ml. Heavy inspiration: Increases anteropost. + vertical dimensions, (exteral intercostal muscles+ diaph.), + elevation of thoracic cage: sternomastoids, scalenes, serratus ant. & pectoralis minor. Heavy expiration: Internal intercostal & abd. m. The alveolar epithelial wall is composed of three types of cells: Type I pneumocytes: Squamous epithelial cells Type II pneumocytes: Secrete surfactant Third type: Alveolar macrophages Home Exit BASIM ZWAIN LECTURE NOTES
Respiration Elastic and non-elastic work Anatomical and physiological dead space Forces controlling lung volumes Lung compliance Pleural pressure (intrapleural pressure) Airways resistance Surface tension and surfactant In restrictive pulmonary diseases (pulmonary fibrosis, pleurisy, pleural effusion….) compliance & tissue resistance work are especially increased while in obstructive airway diseases (emphysema, chronic bronchitis, chronic bronchial asthma….), airways resistance work is especially increased & work of expiration becomes even more than work of inspiration. At rest, only 3-5% of body energy for ventilatory process, rising 50 folds in exercise especially in respiratory diseased subjects. When there is perfusion, but no ventilation, oxyg-enated Bd will be mixed with deoxygenated Bd & condition is called shunt. e.g. of anatomical shunt is oxygenated Bd returned to left atrium via pulm. vv which is mixed with deoxygenated Bd from lung tissues. e.g. of physiological shunt is at base of lung during upright position. Work of breathing is elastic & non-elastic work Elastic (compliance) work: Is work required to overcome elastic forces of lungs & chest (65% of total work). Two thirds of lung elastic forces are due to surface tension & one third is due to elasticity of lung tissues themselves. Compliance work = ΔV . ΔP \ 2 It is the extent to which lung volume expands for each unit increase in transpulmonary pressure. Lung compliance=ΔV\ ΔP where ΔV is change in lung vol. & ΔP is change in transpulmonary pr. Total compliance is about 200 ml\cmH2O, while compliance of lungs & thorax is 110 ml\cmH2O. Compliance is decreased in restrictive pulmonary diseases (pulmonary fibrosis, pleurisy, pleural effusion….) while it is increased in emphysema e.g.s of pathological shunt are congenital anomalies like patent ductus arteriosus (PDA) & patent foramen ovale (PFO). Patent=open. Ductus arteriosus (a bv that allows Bd to bypass baby's lungs before birth) fails to close after birth. Foramen ovale (a normal opening between left & right atria of fetal heart) fails to close after birth Conductive zone is anatomical DS: There is pulm. ventilation but no pulm. Perfusion. When there is alv. ventilation but perfusion temporarily blocked; this is called physiological DS (e.g. at apex of lung during upright position: blood pools into base). When block is permanent, it is pathological DS. Non-elastic work: which is subdivided into: •Airways resistance work: Required to overcome resistance to air movement through respiratory passages which is about 28% of total work •Tissue resistance work: Required to overcome viscosity of lung & chest tissues which is about 7% of total work Pressure that causes alv. collapse is alv. collapse pr. : about 4 cmH2O in presence of surfactant. Alveolar collapse pressure = 2T \ r , where T is surface tension, r is radius of alv. In many premature babies radius of alv. is about 1\4th normal with no secretion of surfactant which increase alv. collapse pr. to 40 cmH2O or more & baby dies from alv. collapse (RDS or hyaline membrane disease). Greatest resistance to air flow is in larger bronchi near trachea (not in smaller airways due to large number of these airways “about 65000 parallel terminal bronchioles” & very small amount of air passing through each. But under certain disease conditions, greatest resistance occurs in smaller airways because they’re occluded by secretory products & greater % of sm. muscles in their walls Direct sympathetic control of bronchiolar smooth muscles is weak but, circulating EPI (& to a lesser extent NE) hormones cause bronchodilatation. Vagal (parasym.) stimulation results in secretion of Ach: causes bronchoconstriction (BC). Atropine (anticholinergic) blocks action of Ach, relieves BC. Irritation of resp. epith. with noxious gases (as SO2) cigarette smoke, fumes, dusts, infection …. results in reflex nervous & local (non nervous) BC Space between visceral & parietal pleurae is filled with pleural fluid: lubrication, sliding & prevents separation. The pressure inside the pleural space is pleural or intrapleural pressure: always negative about -5 to -7.5 cmH2O (1cmH2O = 0.75 mmHg). The pressure inside alveoli is alveolar pressure = about -1 to +1 cmH2O. Difference between pleural and alveolar pressures is transpulmonary pressure. Surface tension is the ability of fluid molecules on surface with air for extra strong attraction resulting in tendency of surface to contract. Surface tension of alv. fluid results in alv. collapse (atelectasis) but this is prevented by presence of a surface active agent secreted by type II alveolar epithelium which is called surfactant. It reduces surface tension from 50 dyne\cm to 5-30 dyne\cm. Surfactant is complex mixture of phospholipids, other lipids, proteins, CHO, Ca++ & some ions. Activity of surfactant depends on conc. & orient-ation of phospholipids molecules on surface, while importance of glycoprotein & Ca++ is to enhance spread of phospholipids over surface. Thyroid & glucocorticoids accelerate maturation of surfactant, cigarette smoking reduces its production. BC is due to allergic reaction (between antibody & antigen) e.g., when histamine, slow reactive substance of anaphylaxis or other substances are released from mast cells in response to exposure to allergens like pollen in air, or other sensitizing agents. This is a type of immune reaction. Home Exit BASIM ZWAIN LECTURE NOTES
Respiration Diffusion of gases Factors affecting diffusion rate Diffusing capacity Henry's law states that partial pr. of dissolved gas is directly proportional to conc. of its molecules & inversely proportional to its solubility coefficient in solvent. Solubility coefficient of CO2 in water is 20 times more than O2 so as diffusion of CO2 across respiratory membrane. Diffusion of gases is along partial pr. gradient (from higher to lower) Partial pr.s of alv. gases are different from inspired gases due to humidification, O2 is continuously up taken to & CO2 is continuously added from pulm. capillary. PO2 of pulmonary vein (95 mmHg) is different from that of pulmonary capillary (104 mmHg) due to anatomic shunt The diffusion rate of O2 is about 230ml\min & 4600 ml\min during exercise. Diffusion rate of gas molecules across biological membranes is affected by several factors summarized in equation: Another factor, temperature which is directly pro-portional to D but it is constant in healthy human A mixture of gases inside a container exerts a total pr. against its walls which equals the sum of partial pr.s of its component gases. Partial pr. of each gas is proportional to its conc. within mixture. Partial pr. of oxygen is PO2, of carbon dioxide is PCO2 & of water vapor is PH2O. Alv. PO2 is PAO2, while arterial PO2 is PaO2 & same thing for CO2. Diffusion of O2 & CO2 across RM takes 0.3 s, while Bd traverses pulm. capillary within 0.75s. at rest. This is called safety factor for exercise when Bd velocity in pulm. capillary becomes 0.3s When Bd is saturated with O2 & CO2 , it must be replaced by perfusion so; uptake of O2 & output of CO2 is perfusion limited. Another toxic gas (CO) has no Bd saturation limits & it is diffusion limited Diffusion rate is greatly reduced in: Pulmonary fibrosis: Increased thickness of RM Emphysema: Decreased surface area of RM High altitude: Reduced pr. gradient of O2 (hypoxia) Diffusing capacity (DL) is vol. of gas diffuses across RM each min. for ΔP = 1 mmHg. At rest, DLO2 =21 ml\min. mmHg & during exercise about 65 ml\min. mmHg (increased Bd flow, ideal distribution & increased surface area of RM due to capillary distension). DLCO2 = 20 times DLO2. Home Exit BASIM ZWAIN LECTURE NOTES
Respiration Ventilation/perfusion ratio Transport of gases to the tissues CO2 is diffused from tissue cells to interstitial space & then through capillary membrane to be dissolved in plasma, but major amount diffuses into RBC to combine with water or Hb to form carbonic acid or carbaminohemoglobin respectively. CO2 + Hb = CO2Hb Carbonic anhydrase (CA) enzyme CO2 + H2O ===================== H2CO3 Carbonic acid is dissociated into bicarbonate & H+ H2CO3 ↔ HCO3- + H+ Gas exchange in pul. capillaries: external respira-tion while in tissue capillaries: internal respiration. About 97% of O2 is transported in combination with hemoglobin (Hb) in RBC & only 3% in dissolved state in water of plasma & cells while CO2 is transported in three forms: - In the form of bicarbonate (HCO3) …. 70% - With Hb & other plasma proteins….... 23% - In dissolved state………………..……... 7% Normal alveolar ventilation/perfusion ratio (VA/Q) is about 0.85 (5100 ml/min/6000 ml\min = 0.85). In blocked ventilation; VA= zero, VA/Q= zero & in blocked perfusion; Q = zero, VA/Q = ∞ In either case there is no gas exchange. In upright position, Bd shifts from top to bottom of lung, so, at top;VA/Q=2.2 & at bottom, VA/Q=0.5 H+ will be buffered with Hb (which is strong acid-base buffer), while HCO3- is antiported with Cl- (chloride shift). This is why venous RBC has Cl- odour & its plasma is alkaline. In pulm. capillary, the events are reversed. Home Exit BASIM ZWAIN LECTURE NOTES
Respiration Carbon dioxide volume percent curve Oxygen-hemoglobin dissociation curve Control of breathing (regulation of respiration) Respiratory quotient Pulmonary receptors 1.Stretch receptors: in bronchial & bronchiolar sm, when lungs overinflate; they overstretch& transmit signals via vagus to DRG, to switch off insp. This is called Hering-Breuer reflex 2.Irritant receptors: cough, sneeze & bronchocons-triction reflexes. Receptors for cough found along bronchial tree (larynx & carina), send impulses via vagus nerve to medulla & sneeze receptors found in nasal airways, impulses via trigeminal to medulla When PO2 is high: favours loading of Hb with O2 (increased % of saturation of Hb with O2) & when PO2 is low: favours unloading of O2 from Hb. The relation between PO2 & % of saturation of Hb with O2 is drawn as O2-hemoglobin dissociation curve: PO2 = 95 mmHg→ 97% saturation PO2 = 40 mmHg→ 75% saturation PO2 = 28 mmHg→ 50% saturation (p50) Decreased p50: shift to left and upward Increased p50: shift to right and downward Respiratory center in the brain stem Respiratory neurons either type I (inspiration) or type E (expiration). Resp. center is composed of several groups of these neurons: 1.Dorsal respiratory group (DRG) 2.Ventral respiratory group (VRG) 3.Pneumotaxic center 4.Apneustic center *Voluntary neural control: directly from cerebral cortex via corticospinal tracts to spinal neurons of resp. muscles. It regulates certain activities like breath holding, hyper-, hypo-ventilation & forceful respiratory maneuvers *Involuntary neural control: Respiratory center (responsible for autonomic resp.) & Pulmonary receptors (responsible for pulmonary reflexes) *Central & peripheral chemical control Bohr's effect states that reduced CO2 & H+ conc. increase O2 binding with Hb in pulm. capillaries & that increased CO2 & H+ conc. increase O2 release from Hb in tissue capillaries. Haldane's effect states that increased binding of O2 with Hb displaces CO2 from Bd in pulm. capillaries to alveoli & that increase release of O2 from Hb will increase CO2 uptake from cells by Bd in tissue capillaries. Peripheral chemical control: pp chemoreceptors, sensitive to changes in PO2, PCO2 and H+. They are: Carotid bodies, aortic bodies & others. Carotid bodies, largest in number, located at bifur-cations of common carotid arteries, afferent signals pass via Hering nerves to IXth cranial nn & then to DRG. Aortic bodies located along arch of aorta & afferent signals pass via Xth cranial nn to DRG. Others are few in number, along large arteries. Control of breathing during exercise When motor cerebral cortex orders muscles to contract; it sends collaterals to respiratory center to increase activity. This may be more or less than actual need. Proprioceptive endings in muscles & joints send impulses to adjust activity but final precise adjustments are by chemical control aided by changes in PO2, PCO2 and H+. Person with pulmonary ventilation of 7.5 L/min breathes 10,800 L of gas each day. From this gas, he takes in 420 L of O2 (19 moles/day)& gives out 340 L of CO2 (15 moles/day). The ratio of CO2 expired/O2 inspired is respiratory quotient (RQ) RQ = CO2 out/O2 in = 340/420 = 0.81 In cellular resp. of glucose, CO2 out=O2 in; RQ = 1 RQ for metabolizing fat is only 0.7, the overall RQ < 1 because diet is mixture of carbohydrates & fat DRG located in nucleus of tractus solitarius & reti-cular substance of medulla, participates in basic resp. rhythm (quiet insp.), only type I neurons VRG located ant. & lateral to DRG in nucleus am-biguous rostrally& nucleus retroambiguus caudally It is inactive during quiet breathing, contributes to resp. control of heavy breathing, receives signals from DRG, contains both types I and E neurons. Factors cause right shift (increased p50) are: 1. Decreased pH 2. Increased CO2 3. Increased temperature 4.Increased DPG (Diphosphoglycerate) This right shifting in tissue capillaries favours unloading of O2 to the tissues When PCO2 increases, vol% of CO2 increases. At PCO2 = 40 mmHg (arterial); vol% = 48 At PCO2 = 45 mmHg (venous); vol% = 52 52% - 48% = 4% (4 ml of CO2 is cleared away from tissue with each 100 ml of blood perfusing that tissue at rest) At PO2= 95 mmHg (arterial)→ 19.4 vol% At PO2= 40 mmHg (venous)→ 14.4 vol% 19.4 – 14.4 = 5 vol%: (5 ml O2 consumed by tissue with each 100 ml of Bd at rest), but during exercise, venous PO2 falls to 15 mmHg at which vol% is 4.4 19.4 – 4.4 = 15 vol%:(15 ml O2 consumed by tissue during exercise) Pneumotaxic center located dorsally in nucleus parabrachialis of pons (Kölliker-Fuse nucleus) & operates in association with apneustic center in lower pons to control depth of insp. They switch off ramp signal of DRG to block over inhalation. The volume of O2 carried by each 100ml of Bd is called vol% which also increases with PO2. In normal subjects, each 100ml of Bd contains 15 g of Hb, & each gram of Hb can bind 1.34 ml of O2 1.34 x 15 = 20 vol% (100% saturation=20vol%) which means when Hb is 100% saturated; 20ml of O2 can be carried by each 100ml of Bd. The opposite factors occur in pulmonary capillaries & cause right shift (decreased p50) which favours loading of O2 to Hb. Presence of large amounts of Hbf (fetal Hb) in Bd is another factor that causes left shift & favours loading of O2 from the maternal circulation to fetal circulation. Fetal Hb has more affinity to combine O2 than adult Hb 3.J-receptors: sensory nerve endings in alv. wall in juxtaposition to pulm. capillaries give the person a feeling of dyspnea during engorgement of pulm. capillaries or edema like in congestive heart failure. Central chemical control: chemosensitive areas of respiratory center, bilateral aggregation of neurons beneath ventral surface of medulla, sensitive to changes in H+ & PCO2, direct stimulus for these neurons is H+, when increased in Bd;the area signal resp. center to increase activity (hyperventilation) In anemic (or polycythemic) patients; Bd contains less (or more) grams of Hb so; vol% is lower (or higher) than 20% at same 100% saturation of Hb. Home Exit BASIM ZWAIN LECTURE NOTES
Respiration Hypoxia Patterns of breathing Low level of PO2 is hypoxia. In blood it is called hypoxemia. Four types of hypoxia: 1.Hypoxic hypoxia: most common, decline in PaO2. 2.Anemic hypoxia: HbO2 is declined due to anemia or CO poisoning. 3.Stagnant hypoxia: blood flow is reduced. 4.Histotoxic hypoxia: tissue can not utilize O2 due to enzymatic inhibition caused by poisons or drugs e.g. cyanide poisoning. Hypoxic hypoxia caused by congenital CV disease (PDA, PFO…), lung failure, pulm. fibrosis, pulm. emphysema, VA/Q imbalance, pump failure (fatigue of resp. muscles, pneumothorax or bronchial obstr-uction) & depression of resp. center (drugs like heroine, morphine, pithidine) … Eupnea: normal rhythmic breathing (12-15 BPM) Apnea: no breathing, dyspnea: conscious shortness of breathing (as in asthma). Hypopnea: decrease (& hyperpnea increase) in rate or depth of breathing regardless of consciousness. If hypo- & hyper-pnea are not with metabolic requirements; they hypo- & hyper-ventilation & lastly tachypnea: rapid shallow breathing. Abnormal patterns of breathing are: 1. Chyne-Stoke breathing: usually seen in patients with brain damage or chronic illness and also in some infants & in healthy persons during sleep especially high altitudes.Characterized by repeated cycles of gradually increasing & decreasing tidal volume & respiratory frequency. 2. Coupled or grouped breathing: in new comers to high altitudes where PCO2 is high & characterized by double, triple or more breaths followed by apnea for several seconds relieved by deep breath. 3. Periodic breathing: in patients with increased intracranial pr. or mid brain lesions & characteri-zed by irregular periods of apnea alternated with periods of normal breathing. 4. Apneustic breathing: in patients with pontine lesions due to loss of pneumotaxic and\or apneustic centers characterized by sustained cramp like insp. efforts relieved irregularly by sudden gasp of deep expiration. Home Exit BASIM ZWAIN LECTURE NOTES