Download
1 / 19
190 likes | 364 Vues
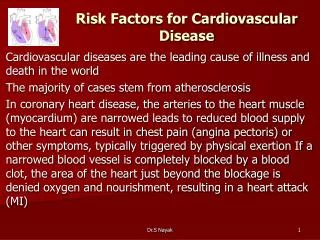
Risk estimation and the prevention of cardiovascular disease SIGN 97. Key messages. Prevention - a journey not a destination Moving from CHD to CVD Risk estimation essential Reinforcement of lifestyle messages Significant changes need to be taken on board.

E N D
Risk estimation and the prevention of cardiovascular disease SIGN 97
Key messages • Prevention - a journey not a destination • Moving from CHD to CVD • Risk estimation essential • Reinforcement of lifestyle messages • Significant changes need to be taken on board
RISK ESTIMATIONThe basis of all rational prevention strategies
CVD PreventionRisk estimation • Multifactorial • Reducing the interventional level to 20% CVD risk in the next 10years • The problem of social deprivation • The potential of a new risk scoring tool: ASSIGN 20
CVD Prevention LIFESTYLE MODIFICATION Diet, exercise, alcohol and smoking remain fundamental!
Lifestyle modification (1) • Diets low in total and saturated fats should be recommended for all for the reduction of CVD risk. (A) • regular physical activity of at least moderate intensity (eg makes a person slightly out of breath) is recommended for the whole populationunless contraindicated by condition . (B)
Lifestyle modification (2) • In patients with no evidence of CHD , light to moderate alcohol consumption may be protective against coronary events. (B) • All people who smoke should be advised to stop and offered support to facilitate this in order to minimise cardiovascular and general health risks. (B) • Motivational interviewing should be considered in patients with cardiovascular disease who require to change health behaviours including diet, exercise, alcohol and compliance with treatment. (B)
CVD Prevention BLOOD PRESSURE LOWERING Lower is better!
Blood pressure lowering (1) • Individuals with BP greater than 160/100 mm Hg should have drug treatment and specific lifestyle advice to lower their BP and risk of CVD. (A) • Individuals with established CVD, who also have chronic renal disease or diabetes with complications, or target end organ damage may be considered for treatment at the lower threshold of systolic >130 mm Hg and /or diastolic >80 mm Hg. (A)
Blood pressure lowering (2) • Asymptomatic individuals with sustained systolic BP >140 mm Hg systolic and /or diastolic BP > 90 mm Hg and whose 10 year risk of CVD is calculated to be: • ≥20% should be considered for BP lowering therapy • <20% should continue with lifestyle strategies and have their BP and total risk reassessed annually (A)
Lipid lowering • All adults over the age of 40 years who are assessed as having a ten year risk of a first CV event ≥ 20% should be considered for treatment with simvastatin 40 mg/day following an informed discussion of risks and benefits. (A) • All patients with established CVD should be considered for more intensive statin therapy following informed discussion. (B) There is no grade A evidence for treating any population to a target TC level
Statins = largest prescribing cost in UK. Statin bill in Lothian = £8.4M (2006)…. Report on Prescribing Pressures in Primary Care 2007-2008. NHS Lothian
Population 787,504 40-74 years 312,097 Eligible for statin • 2o prevn ~15,100 • 1o prevn ~62,000 • Total ~77,100 Receiving statin • Total ~62,000
What does this mean for NHS Lothian? • Around 62,000 patients receiving statin in 2006 • Around 15,000 additional people eligible for statin using new guidance • SIGN approach: majority adequately treated with simva • JBS-2 targets: many will require atorvastatin • Annual cost of treating people newly eligible for statin estimated to range from: • £0.7M (simva) • to £3.5M (atorva) • May be potential to “switch statins” for those already on atorvastatin
Conclusions • SIGN97 provides a summary of the best evidence to date • Evidence does not support “treating to target” (but QOF has target of <5mmol/L) • In Lothian up to 80% of people eligible may already be receiving statins (NB limitations of using prescribing data) • Implementing SIGN97 in Lothian should be affordable (using generic statins)
Implementing the SIGNCVD guidelines Maximise your learning time Key messages for your colleagues
Key messages & beyond (1) • ASSIGN 20 has major implications for primary care, especially practices in deprived areas - is its likely impact deliverable with current resources? • Simva. 40 for all at risk will require increased prescribing resources. • Screening all those over 40 for CVD risk every 5years - this will be extremely challenging given current practice resources? • How can we take on board motivational interviewing within existing resources? • How can we train and supervise people effectively in what should be a widely used practice technique to bring about positive change?
Key messages & beyond (2) • A gradualist approach is required which is multi professional and realistic about the difficulties in relation to practice, resource and capacity. • All colleagues, including secondary care, should be encouraged to take part in learning events which ideally should be in protected time. • Follow up within practices to ensure practice change should be the responsibility of individual CHPs and MCNs.