Download

1 / 23
340 likes | 619 Vues
GISSI-prevenzione. *Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. ANA GARCÍA CAMPOS. MIR IV Cardiología Complejo Hospitalario Universitario A Coruña. AC. GRASOS OMEGA3. Esenciales Poliinsaturados Proporción omega 6:3 ( Para beneficio <= 4:1 ) FUENTES:

E N D
GISSI-prevenzione *Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico ANA GARCÍA CAMPOS. MIR IV Cardiología Complejo Hospitalario Universitario A Coruña
AC. GRASOS OMEGA3 • Esenciales • Poliinsaturados • Proporción omega 6:3 (Para beneficio <= 4:1) • FUENTES: • Pescados: pescado azul • Vegetales: nueces, cañamones, semillas lino • FUNCIONES: • Efectos en membranas • Metabolismo eicosanoides • Transcripción genética Ác. α-linoleico (ALA 18:3n-3) Ác. eicosapentaenoico (EPA 20:5n-3) Ác docosahexaenoico (DHA 22:6n-3)
Efectos observados: antiaterogénicos antitrombóticos antiarrítmicos Posibles mecanismos: Descenso nivel TG Modificación composición de membranas ESTUDIOS PREVIOS: DART (Diet And Reinfarction Trial) Health Professionals Study US Physicians’ Health Study Zutphen study Western Electric study Multiple Risk Factor Intervention Trial Honolulu Heart Program Lyon Diet Heart study AC. GRASOS OMEGA3
α-tocoferol Liposoluble Transportada en LDL-c FUENTES: Aceites vegetales Soja Levadura de cerveza Germen de trigo… FUNCIONES: Antioxidante Antiaterogénica?? Hipótesis modificación-oxidativa LDL-c Apoyado por estudios observacionales de cohortes Resultados contradictorios en ensayos clínicos Nurses’ Health Study Health Professionals’ study Physicians’ Health study ATBC (fumadores finlandeses) CHAOS ? VITAMINA E
Vitamina E y Ac. Grasos poliinsaturados n-3 estudio de efectos sobre mortalidad y morbilidad tras el IAM. Ensayo clínico DISEÑO: prospectivo, multicéntrico (172 centros en Italia) abierto aleatorizado GISSI-PREVENZIONE
11,324 pacientes con Infarto de Miocardio reciente (≤3 meses) Reclutamiento: oct 1993 / sept 1995 Seguimiento: 42 meses. POBLACIÓN EXCLUSIONES • Contraindicaciones a los suplementos dietéticos • alergia conocida a n-3 PUFA o a α-tocoferol • defectos congénitos de coagulación conocidos • Pronóstico desfavorable a corto plazo • Insuficiencia Cardiaca Congestiva manifiesta • Cáncer • Imposibilidad de dar el consentimiento informado escrito • Sin límite de edad.
TRATAMIENTO COMÚN: Tratamiento preventivo recomendado al inicio del estudio AAS β-bloqueantes IECA Dieta mediterránea *Estatinas ¡no apoyadas en evidencia al inicio! TRATAMIENTO DEL ESTUDIO: n-3 PUFA (1 cáps de 1g) 850-882 mg de EPA y DHA diarios (razón EPA/DHA 1:2) *equivalente a 100g pescado azul/día Vitamina E 300mg de α-tocoferol sintético diarios
OBJETIVO PRIMARIO (Combinado) Muerte de cualquier causa, infarto de miocardio no fatal y accidente cerebrovascular no fatal y Muerte cardiovascular, infarto de miocardio no fatal y accidente cerebrovascular no fatal. OBJETIVOS SECUNDARIOS Cada componente del objetivo primario Principales causas de muerte OBJETIVOS
SEGUIMIENTO: A los 6, 12, 18, 30 y 42 meses Reconocimiento médico Analítica lípidos Cuestionario sobre hábitos dietéticos SEGUIMIENTO Y ANÁLISIS • ANÁLISIS • Por intención de tratar • de acuerdo con el diseño factorial (2 grupos) y por grupo de tratamiento (4 grupos).
EDAD SEXO 16.3% 14.7% 85.3% Relativamente POBLACIÓN DE BAJO RIESGO GRADO DE DISNEA FEVI 10.0% 11.6%
DIETA DIETA MEDITERRÁNEA
TERAPÉUTICA TRATAMIENTO MÉDICO
RESULTADOS VARIACIÓN DE NIVEL DE LÍPIDOS EN SANGRE A LOS 6 MESES Diferencia (%) Diferencia (%) Diferencia (%) Diferencia (%)
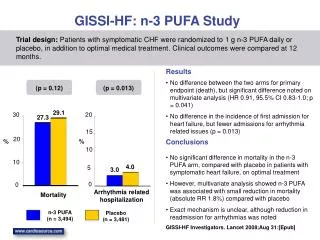
EFECTOS DE n-3 PUFA • Descenso significativo del RR del 10% del objetivo primario combinado “muerte, IAM no-fatal, ACV no-fatal”
EFECTOS DE n-3 PUFA NNT 47’6 50 50 55’6 62’5 RAR 2’1 2’0 2’0 1’8 1’6 • DESCENSO SIGNIFICATIVO DEL RIESGO RELATIVO DE: • 15% de “muerte, IAM no-fatal, ACV no-fatal” • 20% de “muerte cardiovascular, IAM no-fatal, ACV no-fatal” • 20% muertes totales • 30% muertes cardiovasculares • 45% muerte súbita
EFECTOS DE VITAMINA E • Sin evidencia de efecto sobre el objetivo primario o sus componentes individuales • Posible efecto beneficioso sobre muerte cardiovascular y muerte súbita
EFECTOS DE TTO COMBINADO • No beneficio adicional de combinar n-3 PUFA con Vitamina E en mortalidad total/objetivo primario combinado
SUPERVIVENCIA LIBRE DE EVENTOS SUPERVIVENCIA TOTAL
n-3 PUFA disminuyen significativamente la tasa de mortalidad, IAM no-fatal y ACV. Mayor efecto sobre Muerte Súbita Posible efecto directo sobre arritmogénesis necesarios estudios posteriores Ausencia de beneficio sobre eventos atero-trombóticos No se ha objetivado efecto de la Vitamina E. CONCLUSIONES ¡Primer fármaco derivado dietético que demuestra reducción de mortalidad!
n-3 PUFA • Por cada 1000 pacientes/año con IAM tratados 5’4 vidas salvadas MORTALIDAD TOTAL
En prevención secundaria post IAM es recomendación IIb (B) n-3 PUFA 1g al día (actualización Guías del SCASEST de la ACC/AHA 2007) Abiertas nuevas líneas de investigación: Prevención de arritmias fatales y MS En pacientes de alto riesgo portadores de DCI Circulation.2005;112:2762-2768. JAMA.2005;293:2884-2891. JAMA.2006;295:2613-2619. Otros factores dietéticos relacionados J Cardiovasc Med.2007 Sep;8 Suppl 1:S38-41 ACTUALMENTE