Download
1 / 56
812 likes | 1.92k Vues
Oncologic emergencies. Common oncologic emergencies. Mediastinal mass Hyperleukocytosis Tumor lysis syndrome. Other emergencies . Pleural and pericardial effusions Cardiac tamponade Abdominal emergencies Massive hepatomegaly with neuroblastoma Malignant hypertension CNS emergencies

E N D
Common oncologic emergencies Mediastinal mass Hyperleukocytosis Tumor lysis syndrome
Other emergencies • Pleural and pericardial effusions • Cardiac tamponade • Abdominal emergencies • Massive hepatomegaly with neuroblastoma • Malignant hypertension • CNS emergencies • Sepsis
Mediastinal anatomy • PosteriorNeuroblastoma • Middle • Lymph nodes • Anterior • ALL • Lymphoma • Hodgkins • Germ cell tumor Teratoma
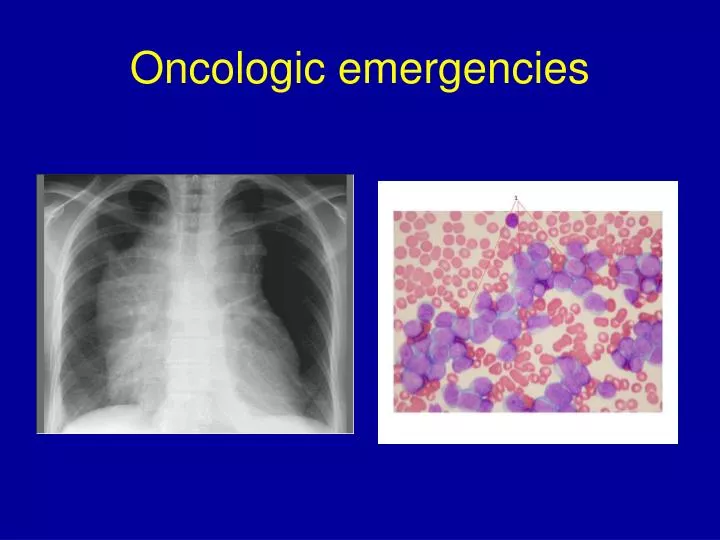
Anterior mediastinal mass Normal mass
Anterior mediastinal mass • What are the risks? • superior vena cava syndrome Tracheal compression • SVC = superior vena cava
Signs and symptoms Cough/dyspnea Dysphagia/orthopnea Wheezing, ↓ breath sounds Dullness to percussion Hoarseness Chest pain Facial swelling, discoloration Remaining PE
Evaluation • Chest xray (Chest CT) • (PA and lateral)
The challenge The need to establish the diagnosis (preferably before treating) The need to treat . . . . . quickly!
Establishing the diagnosis Guiding principles: least invasive testing move quickly CBC, diff, platelets: blasts? Chemistry profile: tumor lysis? Physical exam: lymph nodes to biopsy? Biopsy: bone marrow, lymph node the mass itself
Anesthesia in a child with a mediastinal mass • What is the risk? • Relaxation of chest wall, trachea • Collapse of trachea • Difficult to ventilate • Greater risk with larger masses • Greater risk with greater tracheal compression
Anesthesia in a child with a mediastinal mass • In general, anesthesia should be avoided • Decision should be collaborative with oncologist and anaesthesiologist: • Based on risk of anesthesia • Need for tissue
Treatment of mediastinal mass • Obtain tissue if possible, then treat • Sometimes empiric treatment without obtaining tissue is necessary • Empiric treatment runs risk of obscuring diagnosis • Treatment options • Emergency radiation • Steroid (prednisone, methylprednisolone)
Definition • Peripheral wbc > 100,000/µl • Clinically significant: • > 200,000 in AML • > 300,000 in ALL or CML
Pathophysiology • Due to increased blood viscosity • Adhesive interactions between blast cells and endothelium • Brain and lungs particularly susceptible
Clinical complications • CNS hemorrhage, thrombosis • Pulmonary leukostasis • Metabolic abnormalities
Signs and Symptoms Many children are asymptomatic CNS mental status changes headaches blurred vision seizures coma Pulmonary dyspnea hypoxia cyanosis
Treatment Exchange transfusion is the treatment of choice Avoid blood transfusion right away if hemoglobin is not too low Platelet transfusion is OK IV fluids at twice maintenance Allopurinol Empiric treatment of the leukemia
Tumor lysis syndrome • Metabolic abnormalities that occur as a consequence of tumor cells dying and releasing their contents into the bloodstream
Primary abnormalities ↑ urate ↑ phosphate ↑ potassium ↓ calcium (secondary) ↑ creatinine due to Ca-PO4 precipitation due to urate precipitation
Who is at risk? • Children with tumors with: • high growth fraction • large volume • widely disseminated • sensitive to chemotherapy
Most common malignancies Burkitt’s lymphoma T-cell ALL/lymphoma Other ALL, lymphoma Can happen with any rapidly growing tumor (including solid tumors)
When is the greatest risk? • At presentation • Immediately after starting therapy
Evaluation • In a child suspected of a malignancy: • Extent of tumor • CBC, diff, platelets • Electrolytes • Urate • PO4 • Potassium • Calcium • BUN / creatinine • LDH
Therapy • Hydration is key • D5 ½ NS } • or } 2-4 x maintenance • D5 ¼ NS + 40 mEq/L NaHCO3 } • Do not give potassium • Allopurinol, 300mg/m2/d ÷ t.i.d. • MonitorCheck electrolytes 4 – 6 times a day
Other interventions • For ↑ phosphate • Aluminum hydroxide • Low phosphate diet • For ↑ K • Kayexalate • Calcium gluconate • Insulin
Our approach • Who do we treat? • Any child with ALL, lymphoma, AML • Selected children with large, chemo-sensitive solid tumors • We treat at-risk children even if K, PO4, urate, creatinine are normal
Our approach • How do we treat? • Hydration with D5 ½ NS or D5 ¼ NS + 40 mEq/L bicarb at 2x maintenance • Allopurinol • Rasburicase (selected severe cases) • Laboratory monitoring: 2 – 4 times a day • Continue treatment of the underlying cancer
Summary Physical examination, CXR, and simple blood testing is enough to identify these emergencies. Although tissue diagnosis is preferable before starting treatment, it may not be possible Monitoring with serial laboratory tests is important. Availability of chemotherapy to treat the underlying disease is essential.