Download
1 / 26
300 likes | 639 Vues
Cardiovascular Medications. PICU Resident Talk Stanford School of Medicine Pediatric Critical Care Medicine June 2014. Objectives. Define inotropy , chronotropy , lusitropy , and vasopressor. List the determinants of BP and CO.

E N D
Cardiovascular Medications PICU Resident Talk Stanford School of Medicine Pediatric Critical Care Medicine June 2014
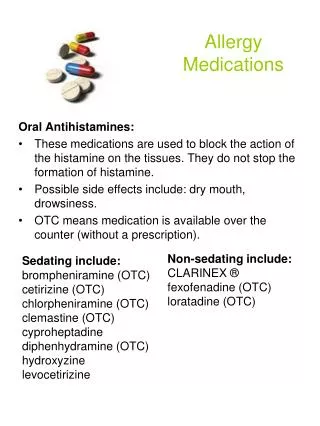
Objectives • Define inotropy, chronotropy, lusitropy, and vasopressor. • List the determinants of BP and CO. • Describe the receptor/ mechanism of action of epi, norepi, dopamine, dobutamine, milrinone, phenylephrine, and nitroprusside. • List the major side effects of these medications.
Definitions • Inotropy—the force of muscle contraction, most commonly cardiac muscle contraction • Chronotropy—affecting the heart rate • Lusitropy—relaxation function of cardiac muscle and chambers • Vasopressor—producing a rise in blood pressure through vasoconstriction
Definitions Bonus ! • Dromotropy • Bathmotropy
Definitions Bonus ! • Dromotropy~ running; increase AV conduction • Bathmotropy ~ threshold; increase excitability of cardiac cells
Chronotropy HR x SV Volume Inotropy EDV - ESV Lusitropy Afterload BP = CO x SVR
Adrenoreceptors vasoconstriction Vascular Smooth Muscle Chronotropy Inotropy Heart vasodilation
Adrenoreceptors β1 receptors: α1 receptors: vasoconstriction Vascular Smooth Muscle Chronotropy Inotropy Heart β 2 receptors: vasodilation
NO & PDE Inhibitors PDE3 Inhibitor: NO → guanalylcyclase: vasodilation Vascular Smooth Muscle Chronotropy Inotropy Heart PDE3 Inhibitor: Vasodilation
PDE Inhibitors PDE 3 PDE 5
PDE Inhibitors PDE 3 PDE 5 Milrinone Sildenafil Tadalafil
Milrinone ↓ SVR ↓ PVR Increases CO Diastolic relaxation Minimal increase HR and O2 demand T1/2 2-4 hrs Further ↑ in renal impairment
Dose: mcg/kg/min Mechanism /Therapeutic Effects Adverse Effects Epinephrine Norepinephrine Dopamine Dobutamine Milrinone Phenylephrine Nitroprusside 0.01- 1 β1 ↑ HR, ↑ inotropy β2 vasodilatation α1 vasoconstriction ↑ SVR Arrhythmia ↑myocardial O2 demand Ischemic injury due to potent vasoconstriction ↑ After load 0.01- 1 α1 vasoconstriction ↑ SVR β1 ↑ HR, ↑ inotropy Min β 2 effects D1 diuresis, natriuresis, renal vasodilatation, (No proven benefit in preventing AKI or ↓ mortality) β1 ↑ HR, ↑ inotropy α1 effects vasoconstriction ↑ SVR < 5 5 -10 >10 Arrhythmia ↑myocardial O2 demand 5-20 β1 ↑ HR, ↑ inotropy Mild β2, α1 antagonist vasodilation ↓ PVR, SVR Arrhythmia, hypotension ↑myocardial O2 demand 0.25 -1 Phosphodiesterase Inhibitor (PDE3 inhibitor): Myocardial : ↑ cAMP ↑contractility + lusiotropy Vasculature: ↑ cAMP vasodilatation ↓ SVR/PVR Hypotension, arrhythmia T1/2 ↑ in renal impairment 0.1-5 α1 vasoconstriction ↑ SVR Ischemic injury due to potent vasoconstriction ↑ afterload 0.1-4 Cyanide toxicity ↑ V/Q mismatch NO activates guanalylcyclase (in vasc smooth muscle) ↑cGMP vasodilation
Chronotropy HR x SV Volume Inotropy EDV - ESV Lusitropy Afterload Dopamine Dobutamine Epinephrine BP = CO x SVR Dopamine Dobutamine Epinephrine Norepinephrine Milrinone Decrease SVR Low dose Epi, Nitroprusside Milrinone Dobutamine Increase SVR High dose Epi Norepinephrine High dose Dopa (>10) Phenylephrine
Some interesting studies… Dopamine increases risk of infections - Inhibits anterior pituitary function & so ↓ prolactin, GH, TSH. 1-3 - Prolactin and growth hormone have immunestimulatory properties.4 - Inhibits lymphocyte proliferation, immunoglobulin synthesis, cytokine production, and promote lymphocyte apoptosis. 5-8 - Chronotropic and inotropic effects increases myocardial oxygen demand, may not be adequately met by coronaries risk of tachycardia and tachy-arrhythmias. 9 - Beta adrenergic properties of dopamine predominate in sepsis10
Some interesting studies… • Septic patients treated with dopamine had a higher incidence of arrhythmias than those treated with norepinephrine.1 • Norepinephrine is a more potent vasopressor than dopamine, with norepinephrine being more effective in reversing the hypotension of septic shock.2 • In patients with sepsis, norepinephrine increases blood pressure, as well as cardiac output, renal, splanchnic, cerebral blood flow, and microvascular blood flow while minimally increasing heart rate.1,3,4 By achieving these hemodynamic goals, norepinephrine may be better than dopamine in maintaining organ perfusion.
We did not talk… • Ionized calcium • Vasopressin • Isoproterenol
Ionized Calcium • Central role in maintaining myocardial contractility • Effects mediated via intracellular concentration, calcium requirements of the muscle cell, sensitivity of the myofilaments to calcium • Agents that increase intracellular cAMP increase intracellular calcium requirements for contraction, thus encouraging smooth muscle relaxation and vasodilation
Angiotensin II Hyperosmolarity Decreased atrial receptor firing sympethatic stimulation Vasopressin Vasoconstriction Renal fluid reabsorption Increased blood pressure
Isoproterenol • Synthetic catacholamine. • Non specific beta, no alpha. • Causes inotropy, chronotropy, and systemic and pulmonary vasodilatation. • Indications: bradycardia, decreased cardiac output, bronchospasm (bronchodilator).
THANK YOU !