Download
1 / 32
340 likes | 519 Vues
Gene therapy and therapeutic gene editing: what are the predictors of success?. Bobby Gaspar Professor of Paediatrics and Immunology Centre for Immunodeficiency UCL Institute of Child Health/Great Ormond Street NHS Trust. Retinal abnormalities. Skin conditions EB. Cystic fibrosis.

E N D
Gene therapy and therapeutic gene editing: what are the predictors of success? Bobby Gaspar Professor of Paediatrics and Immunology Centre for Immunodeficiency UCL Institute of Child Health/Great Ormond Street NHS Trust
Retinal abnormalities Skin conditions EB Cystic fibrosis Haemophilia Severe immunodeficiencies Duchenne’s MD Gene therapy and paediatric conditions Inborn errors OCT, Hurlers X-ALD Fanconi’s anaemia Haemoglobinopathies Acute leukaemias
Primary Immunodeficiency stem cells red blood cell platelets white blood cells neutrophils /monocytes white blood cells / Immune cells
Severe combined immunodeficiency (SCID) Bacteria Fungi Virus Pneumonia, diarrhoea, repeated infections
HSC-multi Molecular defects in SCID SCID/CID c, IL7Ra, JAK3, ZAP-70 RAG1/2, artemis, ligase IV, Cernunnos ADA, PNP MHC I/II, CD3//, CD45, ORAI1 NK T B
Adenovirus Adeno-associated virus Retrovirus How do we get genes into cells? Disabled viruses Non-viral vectors
Blood Bone marrow a g b Stem cells B X X Thymus T In X-SCID growth of lymphocytes is blocked NK lymphocytes Pathology of SCID-X1
LTR-driven gammaretroviral vector: MFG gC Y Q U5 R R U5 MoLV MoLV IL2RG SA SD SCID-X1 gene therapy protocol Criteria for entry: No matched sibling donor Molecularly confirmed diagnosis Common gamma chain vector: PG 13 producer cells (GALV envelope) titre approximately 1x10e6 transducing units per ml
Lymphocyte recovery CD3 P10 P9 P8 P5 P1 T Lymphocytes/µl P7 P6 P3 P4 P2 Weeks
Patient details Age at therapy (months) Maternal graft Mutation Gamma chain expression Total cells infused (x10e6) Current status P1 10 ++ R289X ++ 180 A+W P2 10 ++ S238N - 180 A+W P3 4 - Y125C +/- 78 A+W P4 3y - R289X ++ 115 A+W P5 10 - R222C ++ 200 A+W P6 10 - PolyA - 200 A+W P7 6 - M1i - 84 A+W P8 13 - C182Y + 207 A+W P9 7 - S108P + 160 A+W P10 12 - del - 60 A+W
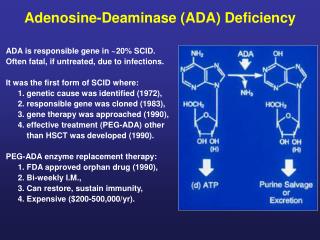
Biochemical defect in ADA deficiency DNA increase is toxic to lymphocyte function d-ATP dCydK d-adenosine d-inosine d-adenosine ADA d-adenosine
Summary of ADA-Deficient SCID Patients Retroviral Vectors, Myeloreductive Conditioning –Milan/London/CHLA-NHGRI, NIH-UCLA 1 As of April 2012 2DFS ≡ Alive without BMT or PEG-ADA re-start Data: Courtesy HB Gaspar (London) and Alessandro Aiuti (Milan)
Patient details Age at therapy (months) Maternal graft Mutation Gamma chain expression Total cells infused (x10e6) Current status P1 10 ++ R289X ++ 180 A+W P2 10 ++ S238N - 180 A+W P3 4 - Y125C +/- 78 A+W P4 3y - R289X ++ 115 A+W P5 10 - R222C ++ 200 A+W P6 10 - PolyA - 200 A+W P7 6 - M1i - 84 A+W P8 13 - C182Y + 207 A+W P9 7 - S108P + 160 A+W P10 12 - del - 60 A+W
Activation of LMO2 Relative to: Leukaemia panel DP1 T cells DP2 T cells Chromosome 11p13 Forward Strand 33.65Mb 33.85Mb 34.05Mb C11orf41 CD59 FBXO3 LMO2 CAPRIN1 NAT10 ABTB2 VIRUS INTEGRATION Fold Difference X
LTR-driven gammaretroviral vector: MFG gC Q Y U5 R R U5 IL2RG MoLV MoLV SA SD New gammaretroviral SIN vectors: Sin11 / SRS11 Q Y R U5 U5 R IL2RG Δ MP Prom. PRE SD RSV EF1(S) SF Development of a new vector for SCID-X1
Reduced mutagenesis with SIN configuration P < 0.001 detection limit 23/24 mice long term survival SF EFS SF.HS
Gene transfer for SCID-X1 using a self-inactivating (SIN) gammaretroviral vector A multi-institutional phase I/II trial evaluating the treatment of SCID-X1 patients with retrovirus-mediated gene transfer Sites: Great Ormond Street Hospital, UK (1) Hôpital Necker Enfants Malades, France (4) Children’s Hospital Boston, US (2) Cincinnati Children’s Hospital Medical Center, US Mattel Children’s Hospital, Los Angeles, US (1)
Phase I/II, non-controlled, open-label, nonrandomised, trial to assess the safety and efficacy of EF1αS-ADA lentiviral vector mediated gene modification of autologous CD34+ cells from ADA-deficient individuals Sites: Great Ormond Street Hospital, UK (2) Mattel Children’s Hospital, Los Angeles, US Vector production: Indiana University Vector Production Facility
Lentiviral vector mediated Gene Therapy for ADA SCID MRC DPFS MRC DCS MRC Research Grant Development of vector Testing of efficacy and safety Phase I/II study of 10 patients December 2012 January 2007 July 2009 January 2018 Collaborations: UCLA Indiana University Vector Production Facility 1st patient treated Feb 2012 3 patients treated in total
Retinal abnormalities Skin conditions EB Cystic fibrosis Haemophilia Severe immunodeficiencies Duchenne’s MD Gene therapy and paediatric conditions Inborn errors OCT, Hurlers X-ALD Fanconi’s anaemia Haemoglobinopathies Acute leukaemias
Gene therapy in PID Cures now available for specific SCID conditions First ever cures with Gene Therapy Morbidity and mortality still low compared to other treatments and prev innovations Need new safer vectors Each disease should be considered individually (gene regulation, expression, tissue specificity)
Many thanks to Institute of Child Health Emma Bjorkeren Kate Parsley Kimberly Gilmour Sam Cooray Elena de Falco Jo Sinclair Doug King Steve Howe Stuart Adams Suzy Thornhill Michelle Quaye Daleen Lopez-Begg Sue Swift Fang Zhang Lin Zhang Claudia Montiel Equiha Maria Alonso-Ferrero Marlene Carmo Christine Rivat Claire Booth Karen Buckland Sue Swift Nourredine Himoudi Anne-Marie McNicol Great Ormond Street Hospital Paul Veys Persis Amrolia Kanchan Rao Graham Davies Alison Jones Cathy Cale Lesley Henderson Jane Gaspar Jin Hua Xu-Bayford Lucie Brown Nursing and support staff Jude Cope Jodi New Collaborators Chris Baum Axel Schambach Christof von Kalle Manfred Schmidt Mik Antoniou Marina Cavazzana-Calvo Alain Fischer David Williams Manuel Grez Vicky Bordon Theoni Petropolou Purine Res Lab, Guys Hospital Lynette Fairbanks Manchester Brian Bigger Fiona Wilkinson Adrian Thrasher Bobby Gaspar





![[V]. Process of Transcription and Transcriptional Control of Gene Expression](https://cdn2.slideserve.com/5058527/v-process-of-transcription-and-transcriptional-control-of-gene-expression-dt.jpg)