Download
1 / 27
270 likes | 389 Vues
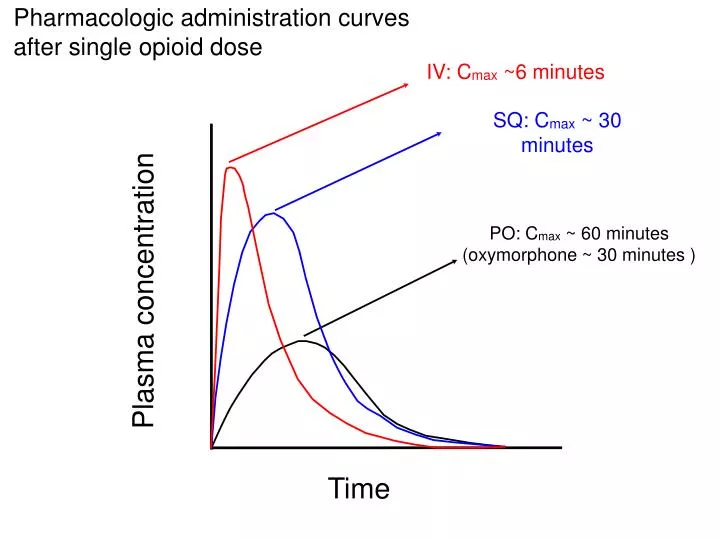
Pharmacologic administration curves after single opioid dose. IV: C max ~6 minutes. SQ: C max ~ 30 minutes. PO: C max ~ 60 minutes (oxymorphone ~ 30 minutes ). Plasma concentration. Time. Opioid infusionsDose escalation. PRN dosing interval based on time to C max:

E N D
Pharmacologic administration curves after single opioid dose IV: Cmax ~6 minutes SQ: Cmax ~ 30 minutes PO: Cmax ~ 60 minutes (oxymorphone ~ 30 minutes ) Plasma concentration Time
Opioid infusionsDose escalation • PRN dosing interval based on time to Cmax: • 1 mg hydromorphone iv Q 10 minutes prn • 1 mg hydromorphone sq Q 15-30 minutes • Despite these efforts Fred continues to have uncontrolled pain. • How rapidly can you safely escalate his continuous infusion and his prn dose?
Opioid infusionsDose escalation • Adjust bolus dose by up to 100% at least every 30-60 minutes until effective • Adjust infusion rate by up to 100% based on prn need every 12-24 hours
The pain crisis • 40 year old man with rectal cancer • S/P abdominoperineal resection • Wound dehiscence • Hospitalized for > 100 days • Daily c/o severe pain • Prescribed 2 mg hydromorphone q 1 hour prn pain • Uncertain how much he had actually been receiving
Methadone • Dual effect • Mu-opioid receptor antagonist (analgesia) • NMDA antagonist (prevention/reversal of opioid tolerance) • Variable equianalgesic ratios
Methadone • 24 hr oral morphine • 0-30 mg • 31-99 mg • 100-299 mg • 300-499 mg • 500-999 mg • > 1000 mg • PO Morphine: Methadone ratio • 2:1 • 4:1 • 8;1 • 12:1 • 15:1 • 20:1
Methadone • Dual affect • Mu-opioid receptor antagonist (analgesia) • NMDA antagonist (prevention/reversal of opioid tolerance) • Variable equianalgesic ratios • Variable metabolism • Half life 8 to 190 hours • Plethora of drug-drug interactions
Methadone • Potent • Effective • Cheap • Complicated • Dangerous
Fentanyl • IV:Transdermal =2:1 • Fentanyl IV: Morphine IV roughly 100:1 • Transdermal absorption dependent on fat stores
Side effects • Constipation • Up to 80 % of patients • Requires stimulant laxatives • Does not abate with time • Counseling important • Nausea • Transient • Vestibular mediated • Responds to anticholinergic anti-emetics • Ondansetron is NOT an anticholinergic antiemetic • Educate patients
Side effects • Pruritis • Transient, responds to antihistamines. • Histamine release is pharmacologic property of morphine • Often misinterpreted as allergic reaction • Urinary retention • Rare but potentially serious
Side effects • Sedation • Especially with initiation or dose increase • Usually resolves • More common with elderly, high dose, polypharmacy • Responds to • Adjuvants/dose reduction • Opioid rotation • Stimulants • Marked sedation requires evaluation
Opioid neurotoxicity • 55 yo old woman with breast cancer • Pain initially controlled on dilaudid 10 mg/hour • Over the past 10 days pain has worsened despite increase in dilaudid to 50 mg/hr. • Patient is anxious, restless. Complains of pain “all over” • Pain elicited by gently stroking arm • Occasional twitching of chest wall and leg noted.
Opioid metabolism • Morphine is metabolized in the liver to: • Morphine-6 glucuronide (Active) • Morphine-3 glucuronide (Neuroexictory) • Excreted in the kidney • Morphine-3-glucuronide accumulates in renal failure, high dose and prolonged therapy, oliguria
Opioid neurotoxicity • Increasing sensitivity to pain (hyperalgesia) • Worsening pain despite rapid opioid escalation • Pain becomes diffuse • Delirium, hallucinations • Allodynia, myoclonus, seizures
Opioid neurotoxicity • Risk factors: • High dose • Morphine>hydromorphone>oxycodone, fentanyl, methadone • Renal failure • Oliguria • Can occur at any dose
Opioid neurotoxicityManagement • Prevention, anticipation, early recognition • Assess urine output, magnesium level, electrolyte abnormalities • Hydration if otherwise appropriate • Opioid rotation at 25% equianalgesic dose • Add NMDA antagonist (ketamine or methadone) • Benzodiazepines/phenobarbital based on severity
Causes of opioid refractory pain • Rapid progression cancer • New source of pain • Abscess • Occult fracture • Bladder outlet obstruction • Pain refractory to opioids (Neuropathic pain, skin ulceration) • Opioid related • Malabsorption, • Drug diversion • Toxicity • Fear, existential or spiritual pain • Delirium
Opioid refractory pain-Management • Opioid rotation or dose escalation • Use of adjuvants, non-opioids • NMDA antagonists (Ketamine and/or methadone) • Address spiritual and psychologic concerns • Non-pharmacologic treatments • Interventional modalities, radiation therapy if appropriate • Consideration of palliative sedation
Barriers to pain relief • Clinician related • Health care system related • Patient related
Patient related • Reluctance to report • “The good patient” • Fear of not receiving chemotherapy • Reluctance to treat • Fears of tolerance • Fear of addiction • Stigma • Meaning of pain • Side effects • “A tradeoff between managing the pain and managing the consequences of managing the pain”
Supporting patient adherence • Normalize concerns • “Some patients worry about becoming addicted or the drug not working in the future when you need it. Are these of concern to you?” • Non-judgmental questioning: • “It must be really hard to take all these pills. How often, in the last week, have you found that you forget one or two?” • Educate and follow up on likely side effects
“Pain is a multifaceted phenomenon involving not only a tissue damage response but also psychological, social, spiritual and existential domains. • (Nessa Coyle, JPSM, 2004)