Download
1 / 33
350 likes | 1.25k Vues
Fungi. 13 Rabiulawal 1430H 10 March 2009. Outline for Medical Mycology. General properties of fungi, growth and isolation Classification of fungi: superficial mycoses, subcutaneous mycoses, endemic (systemic) mycoses Mycotoxins Antifungal chemotherapy Hypersensitivity to fungi.

E N D
Fungi 13 Rabiulawal 1430H 10 March 2009
Outline for Medical Mycology • General properties of fungi, growth and isolation • Classification of fungi: superficial mycoses, subcutaneous mycoses, endemic (systemic) mycoses • Mycotoxins • Antifungal chemotherapy • Hypersensitivity to fungi
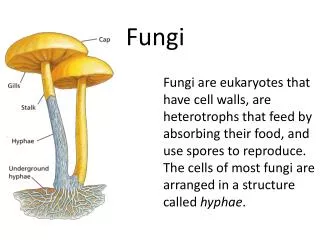
Characteristics • Fungi are eukaryotes with typical eukaryotic structures (nucleus with membrane); cytoplasm contents such as actin cytoskeleton, mitochondria and Golgi apparatus. • Structure: Cytoplasmic membrane of fungi is made of ergosterol, instead of the cholesterol in mammalian cells. Whereas cell wall contains polysaccharides mannan, glucan, and chitin. • Fungal metabolism is heterotrophic, requiring organic carbon, ammonium or nitrate ions for growth. Fungi lack photosynthetic energy-producing mechanism. Strict aerobes or facultative anaerobes. • Size of fungi varies immensely: from bacterial size (2-4µm) to a macroscopically visible structure.
General properties • Reproduction: They produce sexually (spores) or asexually (conidia). • Conidia is an asexual reproductive element; it’s the fungal’s spore-like bodies. • Asexual reproduction – by mitotic division of haploid nucleus, with the production of budding spore-like conidia or separation of hyphal elements. • Sexual reproduction – haploid nuclei of donor fuse with receipient cells and produces diploid cells, may be by meiosis
Fungal Growth and Morphology • Initial growth from a single cell may follow either of 2 courses: yeast or mold. • The first and simplest is the formation of a bud (blastoconidia), extends out from a round or oblong parent, constricts and forms a new cell. Fungi reproduce in this manner are called yeasts. • Mold has tube-like hyphae which consititute their basic structure. Mold develops from hyphal wall. • Reproduction conidia and spores of the molds assume a great variety of sizes, shapes, and relationships to the parent hyphae. Morphology and development of these structures are the primary basis of identification of medically important molds.
Fungal Growth and Morphology • Fungi grow either as yeasts or as molds. The latter show greatest diversity. • Some species can grow either as yeast or mold phase, and are dependent to the environmental conditions. This are termed as dimorphic fungi. • Mold – grow in environmental reservoir and in culture at ambient temperatures. Mold requires minimal nutrients. The conidia produced maybe infectious and serve to disseminate the fungus. • Fungi may then be converted to yeast in infected tissues, for eg. Optimal temperature is 35-37°C.
Classification of Fungi • Morphologically: dependent on the nature of sexual spores and septation of hyphae. • Medically important fungi are grouped based on types of tissues they parasitise and the diseases they produce. • Mycoses: Superficial, cutaneous, subcutaneous, opportunistic, systemic and endemic mycoses.
Glossary 1 • Conidia • Dimorphic fungi
Glossary 1 • Conidia – asexual reproductive structures produced either from the transformation of a vegetative yeast or hyphal cell or from a specialised conidiogenous cell. Microconidia are small, and macroconidia are large or multicellular. • Dimorphic fungi – fungi that have two growth forms, such as a mold and a yeast, which develop under different growth conditions.
Glossary 2 • Hyphae • Mycelium • Mold • Yeast
Glossary 2 • Hyphae – tubular, branching filaments of fungal cells. Most hyphal cells are separated by porous cross-walls or septa. • Mycelium – mass or mat of hyphae, mold colony • Mold – hyphal or mycelial colony of form of growth • Yeast – unicellular, spherical fungal cells that usually reproduce by budding
Diagnosis • In general, fungi are large size, easy for direct microscopic examination of infected pus, fluids or tissues. • Mix specimens with 10% potassium hydroxide (KOH). KOH digests tissue but not fungal cell wall. Visible under microscope with or without stain. • Medium: Sabourand’s agar (glucose and peptones). Blood agar plus antibacterial antibiotics. • Temperature for growth: 25-30°C • Once fungus is isolated, need to identify whether it is a yeast or mold. [Yeast biochemical test analogous to those used for bacteria; mold morphology]. • Dimorphic incubation at 30-35°C; soluble antigens from mycelial growth (exogenous antigen).
Pathogenesis • Less is known about the pathogenic mechanism of fungi compared to bacteria and viruses. • In general, most fungi are opportunists, producing serious disease only in individuals with impaired host defense systems.
Pathogenesis • Yeasts, (eg. C. albicans) are able to colonise mucosal surface of the GI and female genital tracts. • Adhesion Invasion Tissue injury • Invasion through mechanical breaks eg. Sporothrix following a thorn prick. C. albicans undergoes morphologic change, formation of hyphae to penetrate and spread. Extracellular enzymes (proteases and elastases). • Tissue injury mainly due to the inflammatory and immune responses stimulated by prolonged presence of the fungus eg. Dimorphic fungi resist phagocytosis. None by extracellular products or endogenous toxins in a manner analogous to bacterial toxins.
Mycotoxins • Mycotoxins= Exotoxins produced in environment, not in vivo. Produced by a number of mushrooms and molds. • Mycotoxin acts on CNS, liver, GIT, bone marrow or kidney. • Amanita phalloides is the deadliest, whose cap contains enough toxin to kill an adult. • Aflatoxin from Aspergillus flavus, is found in contaminants of grains, corn and peanuts.
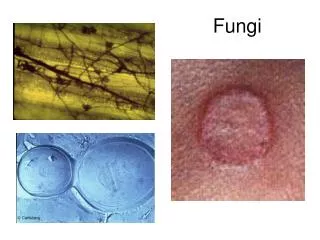
Superficial/Cutaneous Mycoses • Fungi that infect only the superficial keratinised tissue (skin, hair, nails). Not spread to deeper tissues. • Eg. Dermatophytes which cause indolent lesions of skin and its appendages. Dermatophytes are probably restricted to non-viable skin, unable to grow at 37°C or serum +. • Known as ringworm (Tinea corporis)and athlete’s foot (Tinea pedis). • Dermatophyte infections begin after trauma and contact. Moisture, warmth composition of sebum and perspiration, youth and genetic predisposition enhance susceptibility. Incidence higher in hot, humid climates and crowded environment. • Other mycoses: pityriasis versicolor, tinea nigra and piedra.
Subcutaneous Mycoses • Involves dermis, subcutaneous, muscle and fascia. • Fungi normally reside in soil or on vegetation. Enter the skin by traumatic inoculation with contaminated material, followed by subcutaneous spread or lymphatic spread, or both. • Eg. Sporothrix, Chromoblastomycosis, Phaeohyphomycosis and Mycetoma.
Opportunistic Mycoses • Found in normal flora and occasionally produce diseases in compromised hosts. • Candida, aspergillus and related yeasts are endogenous opportunists. Exogenous fungi are present in soil, water and air. AIDS patients are highly susceptible. • Cryptococcus neoformans is characterised by a thick polysaccharide capsule. Very large numbers in dry pigeon faeces. Cryptococcosis is associated with immunosuppressed, AIDS. • Others: mucormycosis and Pneumocystic jiroveci.
Candida • Grow rapidly on Sabourand’s agar and bacteriologic blood agar. • Grows as a yeast with budding, and forms hyphae triggered by changes in condiions such as temperatures, pH, and nutrients. • C. albicans cell wall is made up of a mixture of the polysaccharides mannan, glucan and chitin.
Candida albicans • Is a common member of the oropharyngeal, gastrointestinal, and female genital flora. • C. albicans cause candidiasis – localised disease is seen as erythema and white plaques in moist skin folds or on mucosal surfaces (oral thrush), it may cause itching and thick white discharge.
Pathogenesis • Because C. albicans is regularly present on mucosal surfaces, disease implies a change in the organism, the host or both. The change from the yeast to the hyphal form is strongly associated with enhanced pathogenic potential of C. albicans. • C. albicans hyphae have the capacity to form strong attachments to human epithelial cells via surface hyphal wall protein (Hwp1). • Other mannoproteins may bind to components of extracellular matrix (ECM), such as fibronectin, collagen and laminin. • Hyphae secrete proteinases and phospholipases that are able to digest epithelial cells (and facilitate invasion). • C. albicans has surface receptors that bind to C3, and make it unavailable for opsonisation and resist phagocytosis.
Pathogenesis of Candidiasis • The disruptions of mucosa associated with chronic disease and their treatments (in dwelling devices, chemo) may enhance the invasion process by exposing Candida binding sites in the ECM. • Diabetes melitus also predisposes to infection possibly because of the known greater production of the surface mannoproteins in the presence of high glucose.
Clinical Findings • Superficial invasion of the mucous membrane by C. albicans produces a white, cheesy plaque that is loosely adherent to the mucosal surface. • Thrush occurs on the tongue and palate. Similar lesions are seen in the vagina, known as vaginal candidiasis, a thick, curd-like discharge and causes itchiness of the vulva. • Infection of the UT via haematogenous or ascending routes may (but rarely) produce cystitis, pyelonephritis, abscesses, or expanding fungus ball lesions in the renal pelvis.
Laboratory Diagnosis • Epithelial scrapings and exudate are almost certainly confirmed to have been infected by C. albicans by KOH preparations or Gram smear demonstrate abundant budding yeast cells in the presence of hyphae. • Serological tests to detect C. albicans are so far not sensitive nor specific enough. • Rx: susceptible to amphotericin B, azoles. Superficial infections are treated with topical nystatin or azole. Treating and managing other Candida-associated diseases also help in the recovery.
Aspergillus • Invasive aspergillosis is distinguished by its setting in immunocompromised individuals and its rapid progression to death. Typical patient is one with leukaemia or on immunosuppressants for a bone marrow transplant. • Aspergillus sp. can be found worldwide. They seem to adapt to a wide range of environmental conditions, and the heat-resistant conidia (fungal spores) provide a good mechanism for dispersal.
Pathogenesis • The primary infected organ is the lung. Allergic aspergillosis, which can be a mechanism of exacerbation in patients with asthma, is characterised by transient pulmonary infiltrates and eosinophilia. • Aspergillus conidia are small enough to readily reach the alveoli when inhaled, but disease is rare in normal individuals. • Early factors that initiate fungal infection are unknown.
Diagnosis and Treatment • Aspergillus is relatively easy to isolate and identify, often discovered in invasive disease. • Samples from lung aspiration, bronchoalveolar lavage or biopsy, are analysed for large, branching, septate hyphae. • Serologic methods for Aspergillus antibodies, in non-invasive diseases. • Rx is not effective. Amphotericin B and itraconazole have been used. • Surgical removal of localised lesion is sometimes helpful even in the brain. Constructions of rooms with filtered air has been tempted to reduce exposure to environmental media.
Systemic (Endemic) Mycoses • Most virulent, may cause serious progressive systemic disease. • Cryptococcus neoformans caused cryptococcosis, a chronic meningitis. • Histoplasma capsulatum is a dimorphic fungus that grows in the yeast phase in tissue and mold phase in cultures incubated at 22 to 25°C. Progressive cases of histoplasmosis show extension in the lung or enlargement of lymph nodes, liver and spleen. • Coccidioides cause coccidioidomycosis, often presented as a complex called valley fever by residents of the endemic areas. • Blastomyces
Antifungal Chemotherapy • Many are too toxic for use, poor diffusion into tissues. Superficial topical; systemic toxic antifungal. • Antifungals that affect membrane sterols: • Polyenes nystatin and amphotericin B are lipophilic binds to sterols in cytoplasmic membrane of eukaryotic cells, forms annular channels which lead to leakage of essential molecules… cell death. • Selective toxicity for fungal ergosterol but also binds to cholesterol. • Amphotericin B (AmpB) is insoluble in water, administered as colloidal suspension. • Infusion is followed by chills, fever, headache, dyspnoea and more seriously, renal dysfunction. • Therapy must be titrated against toxicity.
Antifungal – membrane sterols • Antifungals that affect membrane sterols: contd • Azoles: imidazole, ketoconazole, fluconazole, itraconazole. Inhibition of cytochrome enzyme (P450 demythylene). • Many adverse effects but less toxic than AmpB. Azoles is effective for superficial and subcutaneous mycoses. • Allylamines are synthetic compounds, inhibit an enzyme in the early stage of ergosterol synthesis. Rx for dermatophytes ringworm.
Antifungal – Nucleic acid synthesis • Flucytosine (5-Flucytosine) 5FC, is an antimetabolite analog of cytosine, ie. Inhibitor of RNA, DNA, protein synthesis. • 5FC is well absorbed after oral administration, active against C. albicans, C. neoformans. • Limitation is the development of resistance. This is reduced by combination with AmpB.
Antifungal – Cell wall • Echinocandins block glucan synthesis by inhibition of glucan synthetase, cause morphologic disruption and osmotic instability in yeast ≈ β-lactams • Caspofungin against Candida and Aspergillus.