Download
1 / 42
420 likes | 925 Vues
RABIES. Atilla Kiss M.D. Prepared by Kellie Zaylor D.O. January 4, 2006. Epidemiology. In the Third World: An estimated 40-70,000 people die from the disease each year Rare in U.S. 40 cases/year prior to vaccination of domestic animals that began in 1947 3 cases/year now reported.

E N D
RABIES Atilla Kiss M.D. Prepared by Kellie Zaylor D.O. January 4, 2006
Epidemiology • In the Third World: An estimated 40-70,000 people die from the disease each year • Rare in U.S. • 40 cases/year prior to vaccination of domestic animals that began in 1947 • 3 cases/year now reported
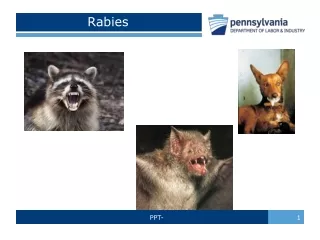
Epidemiology • World wide: Dogs most commonly infected and cause more transmission to humans • Bats: An important source in North & South America and Mexico.
Epidemiology: United States • In U.S.- >90% of rabies occurs in wild animals: Principal reservoirs are racoons, skunks, foxes and bats
Skunks & Racoons • Eastern Seaboard: Rabies is endemic in racoons • Only one human case of rabies from a racoon variant has ever been documented (no history of exposure is known) • North Central, South Central and California: Skunks are important carriers, each with its own regional viral strain
BATS • Rabid bats account for 17% of all cases of rabies in U.S. animals • Hawaii- is rabies-free. There are no rabid bats or rabid terrestrial animals.
Human Cases • Between 1990-2003: 39 cases diagnosed with 32 likely acquired in U.S. • 88% (28 cases) associated with bats • 2 cases associated with the dog and coyote populations of Texas • 1 with a racoon in VA. • 1 with a mongoose in Puerto Rico
Human vs. Bat • In most cases, history of bat contact was obtained after patient’s death. • In 3 cases: victim was aware of the bite, but didn’t seek rabies prophylaxis • In half of cases: victim had bat contact, but no bite history • No history of bat exposure for the remaining victims
Disease Principals • Rabies is not a zoonosis: Animals that get infected will die. • Death occurs within 3-9 days after they first begin secreting virus in their saliva. They can transmit the virus at this point. • Exceptions: Some animals can get sick before virus is found in saliva or may not become ill until several days after virus is secreted.
Disease Principals • Bats can live 10 days after infection • Has been suggested dogs can become asymptomatic carriers, but transmission from one has never been documented • In U.S. all rabid dogs die within 8 days of becoming ill; median 3 days.
Animal Behavior • Classic Picture of rabid, mangy dog foaming at the mouth…not often seen, signs frequently more subtle. • Animals can display aggressive behavior, ataxia, irritability, anorexia, lethargy or excessive salivation.
Animal Behavior • Cats are more likely to be aggressive than dogs • Animals exhibit change in instinctive behavior: nocturnal animal walking around in daylight (i.e. raccoons) • Unprovoked bites
Transmission • Almost all transmission is by bite • 50 times greater risk than a scratch • One human case may have been acquired in a laboratory (transmitted by aerosol)
Transmission • In wild animals: Rabies can be transmitted transplacentally • Transplants in human- possible • Human-to-human: Never has been confirmed • Rabies virus never isolated from blood
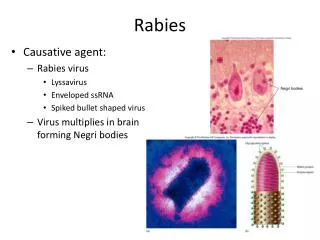
Virus lifestyle • Virus replicated in muscle cells near site of bite for most of incubation time. • Incubation time 30-90 days. Latency up to 7 years • Then ascends along motor and sensory axons at rate of 12-100mm/day and has predilection for brainstem and medulla • Enters salivary glands after replication in CNS.
Rabies virus • Risk of developing rabies after a bite: 5-80%. • Depends upon…. • Severity of exposure • Location of the bite • The biting animal • **Bites on head and neck have shorter incubation time (as short as 15 days) because of rich peripheral nerve supply
Clinical Features • Prodrome: HA, fever, rhinorrhea, sore throat, myalgias, GI upset. *Back pain and muscle spasms. • Agitation and anxiety may result in diagnosis of psychosis or intoxication • Paresthesias, pain or severe itching at site may be the first neurological symptom.
Clinical Features • Over several days symptoms progress • Rabies takes two forms: “Furious”/Encephalitic form: agitation, hydrophobia, extreme irritability, hyperexcitability periods fluctuate with lucidity. • Vitals abnormal: tachycardia, tachypnea, fever
Encephalitic Form • Hydrophobia: Patient can’t swallow because violent jerky contraction of diaphragm and accessory muscles of inspiration when pt attempts to swallow liquids - Patients will be terrified during this reaction and may even experience this at the sight of water or if water touches their face.
Encephalitic Form • Aerophobia: an extreme fear of air in motion can be elicited from some patients. This can also cause violent muscle spasms in the neck and pharynx. • Hallucinations, seizures, ataxia, focal weakness and arrhythmias can occur.
Paralytic Rabies • Other form is “dumb” or paralytic rabies. Similar to Guillain-Barre. • Prominent limb weakness. Consciousness initially spared • Two forms can overlap or progress from one to the other • Coma after one week of neuro symptoms with death a few days after.
Management • Once symptoms occur: fatal in 3-10 days • ICU support: can prolong 4 months. • Six patients have survived clinical rabies: 5 had pre or postexposure prophylaxis before onset of symptoms
Clinical Case • In Wisconsin 2004: 15 year old girl bitten on left index finger by a bat after picking it up off a floor and releasing it outside of her church. • Pt cleaned wound with hydrogen peroxide but did not seek help because the belief that sick/rabid bats could not fly.
Clinical Case • 1 month after bite, c/o fatigue, parasthesias in left hand. Two days later: unsteady, diploplia, nausea/vomiting. • Referred to neuro from pediatrician: MRI/MRA normal and sent home.
Clinical Case • Fourth day of illness: symptoms cont’d. Admitted for LP and supportive care. • CSF: wbc 23 cells • 93% lymphocytes • RBC 3 cells • Protein 50 mg/dL • Glucose 58 mg/dL
Clinical Case • Over next 36 hours: slurred speech, nystagmus, tremors in left arm, lethargy, temp of 102. • Sixth day: bat-bite history reported and rabies considered in differential and transferred to tertiary care center. • Upon arrival: Temp 100.9, impaired muscle coordination, difficulty speaking, double vision, muscle twitching, tremors, obtunded.
Clinical Case • Blood, CSF, nuchal skin samples, saliva submitted to CDC. • Pt developed hypersalivation and was intubated. • Rabies-virus specific antibodies were detected in serum and CSF. No evidence found in nuchal skin biopsies and saliva.
Clinical Case • Management: drug-induced coma and ventilator support for 7 days • IV ribavirin • CSF antirabies IgG: from 1:32 to 1:2,048 • Meds tapered, on 33rd day of illness, extubated, 3 days later transferred to rehab. • Unable to speak, could walk with assistance and feed herself. • Prognosis for her full recovery is unknown.
Management • No effective treatment exists. • Postexposure Prophylaxis/PEP: 3 steps • 1. Wound care: immediate thorough washing with soap and water and a virucidal agent such as povidine-iodine or 1-2% benzalkonium chloride. • Shown to be protective if performed within 3 hours of exposure • If puncture, swab deeply in wound and around edges
PEP • 2. Passive Immunization: Human rabies immunoglobulin (HRIG) 20 IU/kg ASAP, but not longer than 7 days after vaccine given. Infiltrate entire dose around wound, any remaining IG inject IM at a site distant from the vaccine. • 3. Human diploid cell vaccine (HDCV): 1 ml (deltoid) on days 0,3,7,14,28.
PEP • Vaccine: do not give in gluteal. If injected into fat, no antibodies formed. • HRIG and HDCV: give in different anatomical sites and never in the same syringe.
PEP • Local Reactions: itching, erythema, pain, swelling • Systemic: HA, myalgia, nausea. • Anaphylaxis: .1% of cases • Guillain-Barre: 3 cases • Angiodema: 6% of pts who receive boosters. • Can give PEP during pregnancy
Who should get PEP? • Type of exposure • Location of incident (head/neck) • Species of biting animal (common carrier of rabies?)
Significant Exposure • Bites are significant • Nonbite exposures that involve contamination of either mucous membrane or open wound (bled within 24 hours) with saliva • Not significant: petting a rabid animal, contact with its blood, urine, feces. • Skunk spray • Dry virus: NOT INFECTIOUS
Animals in captivity • Wild animals that are caught should by euthanized immediately and head sent under refrigeration to an appropriate lab for testing. • Domestic animals that are apparently healthy should be observed for 10 days. If animal doesn’t become ill, victim does not require treatment. • If animal gets sick, euthanize and test immediately.
References • Chapter 129: Rabies. Rosen’s Emergency Medicine • CDC : http://www.cdc.gov/ncidod/dvrd/rabies http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5350a1.htm • WHO: http://www.who.int/mediacentre/factsheet/fs099/en