Download
1 / 15
150 likes | 167 Vues
Type 2 Diabetes Diet and Exercise Guidelines. Primary Care Clinic Didactic 8/2/19. Outline. Diet Goals Medical nutrition therapy General nutritional considerations Weight loss ADA recommendations Exercise Summary MKSAP question. Type 2 Diabetes.

E N D
Type 2 Diabetes Diet and Exercise Guidelines Primary Care Clinic Didactic 8/2/19
Outline • Diet • Goals • Medical nutrition therapy • General nutritional considerations • Weight loss • ADA recommendations • Exercise • Summary • MKSAP question
Type 2 Diabetes • Accounts for >90% total diabetes prevalence, associated healthcare costs in 2017 were an estimated $727 billion • Although unmodifiable factors such as family history and age partly have a role in the causal pathway of type 2 diabetes, modifiable factors such as lifestyle factors (including diet) contribute to the onset of the disorder as well • Changes in these lifestyle factors can reduce the risk of type 2 diabetes and influence the progression of this disease • This talk will focus on diet and exercise recommendations in patients with diabetes, not for prevention of diabetes
Goals of Medical Nutrition Therapy (MNT) Medical nutrition therapy (MNT) includes a nutrition prescription tailored for people with diabetes based on medical, lifestyle, and personal factors The nutritional goals for people with type 2 diabetes are to: • Maintain blood glucose levels as near-normal as possible by balancing food intake with activity and medications or insulin • Achieve optimal blood pressure and lipid levels • Provide appropriate calories for achieving and maintaining a healthy, desirable body weight • Manage risk factors and prevent complications of diabetes • Address individual nutrition needs, incorporating personal and cultural preferences, willingness to change, and maintenance of the pleasure of eating by restricting choice only when clearly appropriate
Nutritional Considerations for all Weights • Macronutrient composition • Evidence suggests that there is not an ideal percentage of calories from carbohydrate, protein, and fat for all people with diabetes • Must be individualized – Preferences, culture/religion, metabolic goals, SES, comorbidities etc • Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and plant-based diets, ‘diabetes plate’ are examples of appropriate • Nutritional content of foods • Poly or mono unsaturated fats instead of trans fats • No role for supplements • Essentially the same nutritional content recs as general population • Carbohydrate Consistency • Consistency, not content • Timing of food intake
An umbrella review of 53 systematic reviews with meta-analyses that included prospective observational studies focused on type 2 DM association with dietary behaviors • Inverse relationship with fiber intake and modest alcohol intake. Positive association with higher intake of red meat, processed meat, and sugar-sweetened beverages
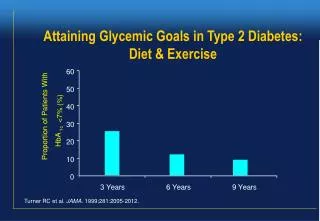
Weight Loss • Improved glycemic control induced by weight loss is associated with partial correction of the two major metabolic abnormalities in type 2 diabetes: insulin resistance and impaired insulin secretion • Caloric restriction, even before significant weight loss, will result in short-term improvement in glycemic controlin the short-term • For patients with type 2 diabetes who are overweight (BMI ≥25 to 29.9) or obese (BMI ≥30), initial recommendations for weight loss are to lose 5 to 10 percent of initial body weight • Patients need not reach ideal body weight to achieve improvement in health status, particularly if the patient engages in regular exercise
Weight Loss Strategies • No One-Size-Fits-All Strategy • A weight loss of >6 kg (approximately a 7–8.5% loss of initial body weight), regular physical activity, and frequent contact with RDs appear important for consistent beneficial effects of weight loss interventions than specific pattern • Multiple weight reduction strategies have been studied in patients with T2DM, no one has shown clear superiority, but when weight loss was achieved, there was improvement in glycemic control in multiple studies • Counting calories and fat grams • Meal replacement • Exchange system approach • Bariatric surgeries, medications • Exercise
ADA Recommendations • An individualized MNT program, preferably provided by a registered dietitian, is recommended for all people with type 1 or type 2 diabetes or gestational diabetes mellitus • Monitoring and insulin adjustment for carbohydrate intake • A variety of eating patterns (Mediterranean, low fat, low carbohydrate, vegetarian) are acceptable. • Trans fatty acid consumption should be kept as low as possible. • Protein intake goals should be individualized but not lower than 0.8 g/kg body weight per day • Fiber intake should be at least 14 grams per 1000 calories daily; may improve glycemic control • A reduced sodium intake of 2300 mg per day with a diet high in fruits, vegetables, and low-fat dairy products is prudent • Sugar-sweetened beverages should be avoided • Sugar alcohols and non-nutritive sweeteners are safe when consumed within daily levels established by the US Food and Drug Administration (FDA).
Hypoglycemia Avoidance • For individuals on a fixed daily insulin schedule, meal planning should emphasize a relatively fixed carbohydrate consumption pattern with respect to both time and amount • It is not advised to use protein to treat hypoglycemia or to prevent hypoglycemia • Avoid alcohol – can cause delayed hypoglycemia
Exercise • Exercise has been shown to improve blood glucose control, reduce cardiovascular risk factors, contribute to weight loss, and improve well-being. • Structured exercise interventions of at least 8 weeks duration have been shown to lower A1C by an average of 0.66% in people with type 2 diabetes, even with-out a significant change in BMI • Higher levels of exercise intensity are associated with greater improvements in A1C and in fitness
Exercise Recommendations • Adults with diabetes are encouraged to perform at least 150 minutes of moderate-intensity (eg, brisk walking) aerobic exercise per week, distributed over at least 3 days • T2 diabetic should also be encouraged to perform resistance training at least twice per week (in absence of contraindications –ie mod-severe proliferative retinopathy) • Vigorous exercise should be avoided in the presence of ketosis but it is not necessary to defer exercise based on mild hyperglycemia (BS<250) • No need for exercise stress testing; start gradually and ramp up • Adjustments of their insulin regimen before, during, and after exercise are recommended; changes in blood glucose can be documented and then predicted for subsequent exercise sessions
Hypoglycemia Avoidance • Hypoglycemia is uncommon in patients with type 2 diabetes not treated with insulin or insulin secretagogues • Self-titration of insulin by blood sugar checks before, during and after exercise • Reduce meal time doses of insulin prior to activity • For at risk patients, or with pre-activity BS<100, eat 15-30 g carbohydrate load 15-30 min prior to initiation • Maintain fluid intake • Decrease the insulin dose that affects time of the day when exercise will be performed by approximately 30 percent • inject the insulin in a site other than the muscles to be exercised
MKSAP • A 40 year old man with type 2 diabetes presents to the office. He seeks advice on his diabetes management as he intensifies his exercise routine in preparation for a a 10K race. He reports prolonged hypoglycemia during intensive exercise , despite eating a meal prior to activity. His insulin regimen is glargin and glusiline. His most recent Hba1C% was 7.0. Which of the following is the most appropriate management • A. Decrease meal-time insulin prior to exercise, continue glargine • B. Discontinue glargine, continue glusiline • C. Increase meal-time protein prior to exercise, continue current regimen • D. Switch insulin glusiline to a sliding scale regimen, continue glargine
Citations • American Diabetes Association. 4. Lifestyle Management: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018; 41:S38. • American Diabetes Association. Nutrition Recommendations and Interventions for Diabetes: a position statement of the American Diabetes Association. Diabetes Care 2007; 30 Suppl 1:S48. • Franz MJ, VanWormerJJ, Crain AL,et al. Weight-loss outcomes: a systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc 2007;107:1755–1767 • Look AHEAD Research Group, Wing RR, Bolin P, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med 2013; 369:145. • NeuenschwanderM, Ballon A, Weber KS, Norat T, Aune D, Schwingshackl L, Schlesinger S. Role of diet in type 2 diabetes incidence: umbrella review of meta-analyses of prospective observational studies. BMJ. 2019 Jul 3;366:l2368. doi: 10.1136/bmj.l2368. Review.