Download
1 / 25
280 likes | 645 Vues
Preparation for IVF. Ian Cooke Emeritus Professor University of Sheffield Director of Education International Federation of Fertility Societies. Precongress seminars XIХ International conference of RAHR “Reproductive technologies today and tomorrow” September , 10-12, 2009

E N D
Preparation for IVF Ian Cooke Emeritus Professor University of Sheffield Director of Education International Federation of Fertility Societies Precongress seminars XIХ International conference of RAHR “Reproductive technologies today and tomorrow” September, 10-12, 2009 Irkutsk, Siberia
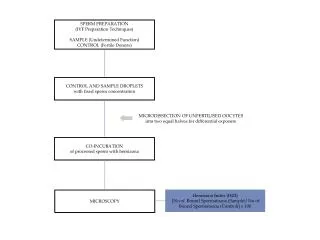
Preparation for IVF Of the patients Of staff and facilities Of organisation • Review of U.K. infertility Guideline algorithm (2004, but valid) • Emphasis on process leading to IVF
U.K. National Guideline developed by a multidisciplinary group: Stages 1. Process published 2. Draft formulated 3. Professional consultation with interested bodies 4.Modification 5. Final publication
Background • The Guideline was produced for the NHS because of the wide variation in and limited access to NHS treatment. It covered a new review of the research evidence. • The National Institute for Clinical Excellence (NICE) Guideline was “to offer best practice advice on the care of people in the reproductive age group who perceive that they have problems in conceiving” (Feb.2004) • Based on the Management of Infertility (RCOG,1998-2000) : initial (primary) investigation and management, management in secondary care and management in tertiary care. The full Guideline (CG11, 500pp. with refs)“Fertility assessment and treatment for people with fertility problems” is available (as a 1.21Mb file) at: http://www.nice.org.uk/guidance/index.jsp?action=download&o=29269
Algorithm for assessment and treatmentfor people with fertility problems (NICE) • Definition of infertility - 2 years • Initial advice to people concerned about conception • Early investigation - history of predisposing factors - woman’s age ≥ 35y - HIV status - hepatitis B & C • People preparing for cancer treatment (oocyte cryopreservation) • Principles of care - Couple centred management - Access to evidence-based information (verbal and written) - Counselling from someone not directly involved in management of the couple’s infertility - Contact with fertility support groups - Specialist teams
Initial advice -1 Cumulative probability of pregnancy in the general population Fertility declines with a woman’s age • Lifestyle advice Preconceptual advice -folic acid, rubella, cervical screening
Initial Advice - 2 • Intercourse at least every 2-3 days C • Alcohol not >2-3U/day (F) D not >3-4 U/day (M) GPP excess alcohol is detrimental to semen quality B • Smoking may reduce fertility in females, refer to cessation programme A • Smoking in males: no link, but stopping will improve general health GPP • Passive smoking may reduce fertility B • No consistent evidence about caffeinated beverages (tea, coffee, cola) B • BMI ≥30 (F), if anovulatory, lose weight, preferably in a group A • BMI ≥30 (M) is likely to be associated with reduced fertility C • BMI <18 with irregular menses should gain weight B
Clinical investigation and management strategy for the male Semen analysis (WHO) If abnormal If normal, see female / unexplained infertility • Hypogonadotrophic hypogonadism: • Gonadotrophins Obstructive azoospermia: Surgery Sperm recovery Mild male factor fertility problems: Unstimulated IUI x 6 cycles Varicocele(s): NOSurgery Failure of IUI IVF Ejaculatory failure: Drug therapy Sperm recovery IVF IVF IVF
Assessment of ovulation • Day 21 Serum progesterone (may be later) • Serum gonadotrophins, FSH and LH • Noprolactin, unless galactorrhoea or pituitary tumour • Noinhibin B; no thyroid function tests unless symptoms of thyroid deficiency • Noendometrial biopsy
Irregular ovulation • WHO Group I - gonadotrophins with LH activity - pulsatile LH • WHO Group II - mainly PCOS Clomiphene - if anovulatory on clomiphene, hMG oruFSH or rFSH with ultrasound monitoring Hyperprolactinaemia -bromocriptine
Tests for tubal occlusion • Semen analysis and ovulation data should be known • Screen for Chlamydia trachomatis before uterine examination or prophylactic antibiotics • HSG or Hysterosalpingo-contrast- ultrasonography if no history of endometriosis or pelvic inflammatory disease or ectopic • Laparoscopy and dye if history of co-morbidity
Female Consider: • If occlusion, - IVF - tubal surgery if mild disease - tubal catheterisation or cannulation if proximal occlusion • If minimal/mild endometriosis - Surgical ablation or resection and adhesiolysis at laparoscopy - If no pregnancy - Stimulated IUI for 6 cycles with ultrasound monitoring with risk of OHSS and multiple pregnancy • If moderate/severe endometriosis - surgery • Endometriomas - laparoscopic surgery
Unexplained infertility • If normal: Unexplained infertility (normal semen analysis, no ovulation disorders, no tubal occlusion) • clomiphene citrate • unstimulated intrauterine insemination (IUI) • Fallopian tube sperm perfusion
Factors affecting outcome of IVF • Salpingectomy before IVF for women with hydrosalpinges • Optimal age 23-39 years • Increased success with previous pregnancy and/or live birth • Ideal Body Mass Index is 19-30 • Increased success with low alcohol/caffeine intake • Increased success in non-smokers • Consistent outcome for first 3 cycles of treatment, effectiveness after 3 cycles is uncertain
IVF • If no pregnancy with oligozoospermia, bilateral tubal occlusion or 3 years’ infertility and the woman is aged 23-39 years: offer up to 3 cycles of IVF • Additional principles of care: • Access to evidence-based information (verbal and written) on risks/implications of assisted conception, including health of resulting children; genetic counselling; consideration of welfare of the child
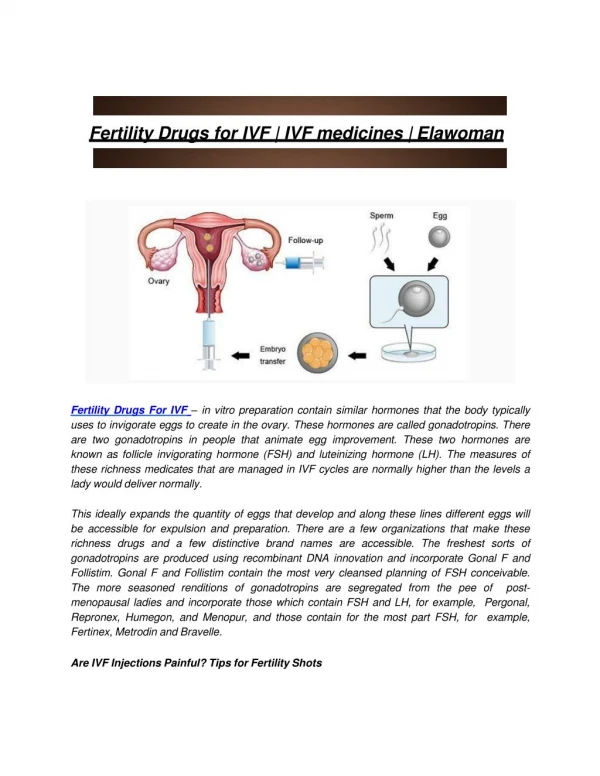
Procedures in IVF treatment - 1 • Offer screening - HIV, hepatitis B, C, specialist referral if positive • Ovulatory stimulation - Nonatural cycle - GnRH agonist down regulation or agonist with gonadotrophins to reduce cost - No antagonists, noGrowth hormone - Monitor follicular development with ultrasound: have a protocol to manage OHSS - Oocyte maturation with hCG - Oocyte retrieval: offer conscious sedation - Nofollicle flushing, noassisted hatching
Procedures in IVF treatment - 2 • Embryo transfer - Not >2 transferred in any one cycle - Offer cryostorage if >2 embryos - Frozen embryos to be transferred before further stimulated cycle - Ultrasound guided embryo transfer on day 2 or 3, or day 5 or 6 • Luteal support - progesterone
Management options with IVF or other forms of ART - 1 • ICSI - Severe semen defects, azoospermia - Poor IVF treatment response - Screen by karyotype • Donor insemination - Azoospermia - Genetic disease in male partner - Severe rhesus isoimmunisation - Severe semen defects For female: - Confirm ovulation, HSG if no pregnancy after 3 cycles
Management options with IVF or other forms of ART - 2 • Oocyte donation - Premature ovarian failure - Gonadal dysgenesis including Turner syndrome - Bilateral oophorectomy - Ovarian failure following chemo- or radio-therapy - Some cases of IVF treatment failure - Gene disorder transmission to offspring - Screen donors - Risks of ovarian stimulation and egg collection • Egg sharing - counselling
Key priorities in infertility management (3/6) before IVF Assessing tubal occlusion and uterine abnormalities • Screen for Chlamydia before uterine instrumentationB (A key priority) • If positive, treat and refer the sexual partner for screening C • Consider prophylactic antibiotics before uterine instrumentation if not screened GPP • If no co-morbidities (pelvic inflammatory disease, previous ectopic, endometriosis) offer HSG (hysterosalpingogram [or hysterosalpingo- contrast-sonography] A) to screen for tubal occlusionB (A key priority) • If co-morbidities, offer laparoscopy B • Hysteroscopy should be clinically indicated and not used routinely. Treatment of uterine anomalies is not clearly linked to fertility B • Do not use routine post-coital testing of cervical mucus as it has no predictive value for pregnancy rate A
Intrauterine insemination • Mild male factor, unexplained infertility and mild to moderate endometriosis should have 6 cycles of IUIA (A key priority) • It should be unstimulated IUI in male factor and unexplained infertility A • Use stimulated IUI for mild to moderate endometriosis A • Use single insemination (A) and Fallopian tube perfusion A
Secondary Care Initial investigations Pelvic assessment Patient choice of management Support services Ovulation induction Unexplained infertility Endometriosis Tertiary Care Location of Services Organisational and management responsibility Quality management Resource management Assisted conception services Gamete donation Evaluation and improvement Continuing professional development BFS/RCOG Standards of Care Summary And so on… through secondary and tertiary care; also providing auditable standards for the Clinic, the Andrology lab and the Assisted Reproduction clinic
CONCLUSION • A great deal of preparation is required before IVF can be implemented: - agreed protocols - informed staff - patients prepared factually and emotionally - Efficient, responsible organisation