Download
1 / 16
171 likes | 367 Vues
A Rare Case Of Parotid Dermoid. Dr. Nikesh M Gosrani PG RESIDENT, IGGMC, NAGPUR. HISTORY. 19 yr old male c/o swelling on right parotid region since 9 years Increasing gradually. HISTORY. Past history - not significant Family history - not significant

E N D
A Rare Case Of Parotid Dermoid Dr. Nikesh M Gosrani PG RESIDENT, IGGMC, NAGPUR
HISTORY • 19 yr old male • c/o swelling on right parotid region since 9 years • Increasing gradually
HISTORY • Past history - not significant • Family history - not significant • Personal history - chronic gutka chewer
GENERAL EXAMINATION • GC- mod • Afebrile • P-74/min • BP- 120/80 mmHg • No pallor/clubbing/cyanosis/icterus/edema • No significant cervical lymphadenopathy
Systemic Examination • Respiratory system -NAD • Cardiovascular system - NAD • Gastrointestinal system - NAD • Central Nervous System - NAD
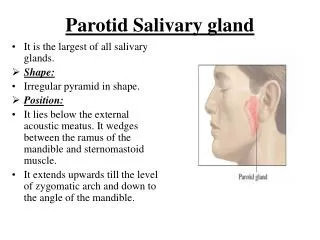
LOCAL EXAMINATION • Swelling in rt parotid • size 4x3cm • Soft ,cystic ,mobile non • Fluctuant • No s/o inflamation • Overlying skin normal
LOCAL EXAMINATION • Facial nerve normal examination b/l • Oral cavity -NAD • Nose -NAD • Ear -NAD
INVESTIGATIONS • Hb - 12.9 gm% • TLC - 8800/mm N-56%,L-38%,E-3%,M-3% • Bld. Urea - 16 mg% • Urine – N.
FNAC - inconclusive • USG LOCAL- mild heterogenous lesion in right parotid size 4x3x4 cm on superficial lobe ? Pleomorhic adenoma • Differential Diagnosis : Rt parotid pleomorphic adenoma Warthins tumor DermoidBranchial cleft cyst Branchial pouch cyst • Advice operation :superficial parotidectomy
Intraoperational findings : • Mass 4x3x4 • Unilocular cyst • Opaque grey white • Dense fibrous wall
Histopathology report : • Cyst wall - stratified squamous • Underlying sebaceous glands • With hair follicles • s/o d=Dermoid
Discussion • Also called Epidermal cyst. • Dermoid cyst of head & neck rare (6.9% of all dermoid cyst) Orbit 49.5%, nose 12.6%, submental & submaxillary region 23.3 % remainder 14.6% • Initially Based on pathogenesis & microscopic appearance • Congenital dermoid - teratoma type(ovaries & testes) • Acquired dermoid cyst (hands & other exposed parts) • Congenital inclusion dermoid (head & neck). a.nasooptic groove b.nose (frontonasal plate) c.submental & submaxillary region d.miscellaneous group(midventral or middorsal line )
Discussion • Now 4 types of Dermoid – Sequestration dermoid Implantation dermoidTubulodermoidTeratomatousdermoid • Sequestration – inclusion of epithelium burried at line of embryonic fusion eg; near head & neck • Implantation dermoid- indriven epithelium beneath skin due to puncture injury eg ; exposed part of body • Tubulodermoid– cyst from unobliterated portion of congenital ectodermal duct or tube eg;thyroglossalcyst,post anal cyst,ependymal cyst in brain • Teratomatoiddermoid – from totipotent cells eg; ovary,testis
Discussion • Parotid dermoid – rare entity • Clinicallydifficultto make diagnosis • Physical examnation – no characterstic findings • Isolated mass, near surface or within gland • Histologically –keratization of squamous epithelium, a/w skin appendages – hair follicles,sweat glands, sebaceous gland • Parotid dermoid relatively well encapsulated • Simple excision may recur so superficial parotidectomy is advisable
Conclusion • Parotid extremely rare • Due to rarity & absence of pathognomonic findings , difficult to diagnose preoperatively • Must be differentiated from malignant tumors & other cystic lesion • Recur after simple excision so superficial parotidectomy is advisable