Download
1 / 49
490 likes | 622 Vues
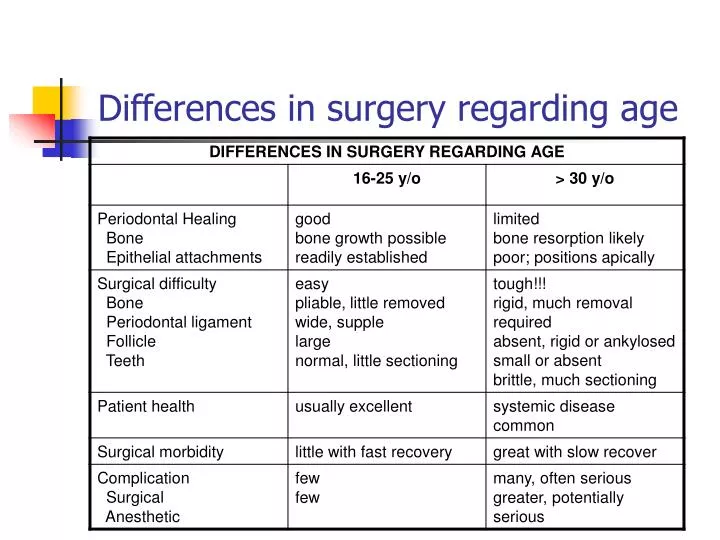
Differences in surgery regarding age. Lecture 2. Objective is to familiarize and help understand Classification of third molar Assess degree of difficulty while performing the procedure. Predicting Difficulty. Accessibility (Risk evaluation factors) Radiographic evaluation

E N D
Lecture 2 • Objective is to familiarize and help understand • Classification of third molar • Assess degree of difficulty while performing the procedure
Predicting Difficulty • Accessibility (Risk evaluation factors) • Radiographic evaluation • Location of the IAN • Third molar position-Angulation • Bone mass density • Clinical evaluation • Age • Obesity • Large tongue • Dilacerated roots • Strong gag reflex • Complaining patient • Surgical access space • Interincisal opening
Ideal time for extraction of Impacted teeth • Average age: 20years • Ideal time for extraction • When the roots are 1/3 formed and before they reach 2/3 formation • Early removal • Low morbidity • Tolerate procedure better • Quick recovery
Classification • Winter 1926 • Based on the position of their long axis in relation to the long axis of the second molars • Angulation and Position • Vertical • Mesioangular • Horizontal • Distoangular • Buccoangular • Lingoangular • Inverted • Unusual
Angulation- Mesioangular • When the third molar is titled towards the second molar in a mesial direction • Most common • 43% of impacted teeth
Angulation- Vertical • Long axis of the third molar runs parallel to the second molar • Second largest frequency-38%
Angulation- Horizontal • Long axis of the third molar perpendicular to the second molar • More difficult to remove • 3% of all mandibular impactions
Angulation- Distoangular • Long axis of the third molar is distally or posteriorly angled away from the second molar • Most difficult-(runs into the ramus of the mandible)
Comprehensive classification • Based on Pell and Gregory and includes a portion of George B. Winter’s classification is most comprehensive: • A. Relation of the tooth to the ramus of the mandible and the second molar (class I,II,III) • B. Relative Depth of the third molar in bone • (Position A, B,C) • C. The position of the long axis of the impacted Mandibular third molar in relation to the long axis of the second molar (from Winter’s classification)
Relation of the tooth to the ramus of the mandible and the second molar • Class I : There is sufficient space between the ramus and the distal side of the second molar for accommodation of mesiodistal diameter of the crown of the third molar
Class II • The space between the ramus and distal side of the second molar is less than the mesiodistal diameter of crown of the second molar
Class III • Class III : All or most of the third molar is located within the ramus
Relative Depth of the third molar in Bone • Position A: The highest portion of the tooth is on a level with or above the occlusal line
Relative Depth of the third molar in Bone • Position B: The highest portion of the tooth is below the occlusal plane, but above the cervical line of the second molar
Relative Depth of the third molar in Bone • Position C: The highest portion of the tooth is below the cervical line of the second molar
Other difficulty factors • Root Morphology • Length • Conical or fused roots • Divergent • Curvature • Direction • Number • Width • Periodontal ligament space
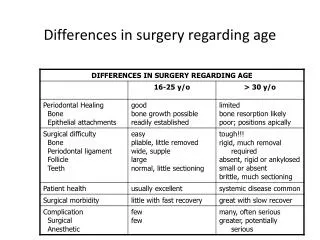
Size of the follicular sac • Wide- (almost cystic) • Extraction is easier • Less bone removal • Younger patients • No Space • Difficult extraction • More bone removal • Older patients
Density of Bone • Age determining factor • 17-25years favorable for extraction • Less dense • More pliable, Expands easily • Easy to cut with a dental bur • >35years unfavorable for extraction • More dense • Decreased flexibility, does not expand • Difficult to cut with a dental bur
Other factors of difficulty • Relationship with IA nerve • Close proximity with the roots • Damage • Parasthesia or anesthesia of the lower lip and chin on the affected side
Other factors of difficulty • Contact with Mandibular second molar • Cautious with Horizontal and distoangular extraction • Safe application of elevators • Check for large restorations, crowns, endodontic treatment on second molars
Nature of Overlying Tissue • Soft tissue impacted • Height of the contour of the tooth is above the level of the alveolar bone and the superficial part of the tooth is covered with soft tissue
Nature of Overlying Tissue • Partial bony impacted • Superficial portion of the tooth is covered by soft tissue but at least a portion of the height of contour of tooth is below the level of the alveolar bone.
Nature of Overlying Tissue • Full bony impacted • Completely encased in the bone.
Why is Buccal position easy • Accessibility-Good • Accessibility-Better instrumentation • Overlying Bone • Lower surgical morbidity
Why is Palatal impaction difficult ? • Accessibility-Poor • Accessibility-Poor instrumentation • More bone removal • High surgical morbidity
Difficulty factors specific to Impacted Maxillary 3rd Molars • Maxillary Sinus • Roots are in intimate contact • Tooth may form the posterior wall of sinus • Sinusitis • Oroantral communication • Maxillary tuberosity fracture • Dense, non elastic bone • Large maxillary sinus • Divergent roots • Mesioangular impactions • Excessive force
Impacted Maxillary Cuspids • Positioning in the alveolar process • Labial • Palatal • Middle
Impacted Maxillary Cuspids –Degree of Difficulty • Based on determination of position • Labial (easy) • Palatal (difficult)/Middle (difficult) • Potential damage to adjacent teeth • Potential Periodontal deficits due to bone removal
Impacted Maxillary Cuspids • Treatment Options • Wait and watch • Surgical extraction • Surgical exposure with Orthodontic movement in Arch
Thank you!! Have a Great weekend!