Download
1 / 21
210 likes | 469 Vues
Otitis & pharyngitis in children. Chap. 121. Otitis media. Acute OM (suppurative, purulent, bacterial) - Inflammation of middle ear OM with effusion (serous, secretory, nonsuppurative, mucoid) – relatively asx collection of fluid in middle ear

E N D
Otitis & pharyngitis in children Chap. 121
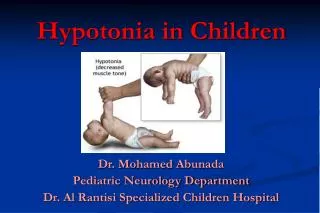
Otitis media • Acute OM (suppurative, purulent, bacterial) - Inflammation of middle ear • OM with effusion (serous, secretory, nonsuppurative, mucoid) – relatively asx collection of fluid in middle ear • Acute( < 3 wks), subacute (3 wks – 3 mos), & chronic (> 3 mos) • Hearing loss can be present with either
Acute OM • Middle ear effusion can persist for wks to mos • Axbx just gently sterilize the effusion but do not clear it from the middle ear space • Most common orgs • S. pneumo • H. flu • M. cat • Dz can occur as a result of eustachian dysfxn • Obstruction • Abnormal patency
Acute OM • Clinical features • Otalgia • Otorrhea • Fever • Remove cerumen before visualizing external canal & TM • TM is usually opaque, pale yellow, red, bulging, bony landmarks obscured • Loss of or decrease in mobility of TM • Aspiration of middle ear is definitive (not practical in ED)
Acute OM • Treatment (table 121-1 & 2) • Amoxicillin (still the DOC); CDC recommends high dose therapy b/c of emerging resistance (80-90 mg/kg/d) • Fig 121-1 (algorithm for guiding drug therapy for AOM) • If infant < 2 wks, then full sepsis w/up and admission for IV axbx • 5-7 d course if > 2 yo • 10 d course if < 2yo, TM perforation, coexisting medical problems, pts at high risk for treatment failure, pts with chronic or recurrent OM • Topical analgesic (Auralgan); do not use if TM perforation present • Acetaminophen & ibuprofen PO
Recurrent AOM • 3 or more episodes of AOM in 6 mos; or, 4 episodes in 12 mos w/ at least 1 episode in last 6 mos • These pts at high risk for hearing loss & speech impairment • Require thorough work-up (ENT ref.) • Prophylaxis w/ axbx (amox, sulfasoxazole); esp in fall/winter
Persistent AOM • AOM w/in 3 days of initiating therapy or recurrence of s/sx w/in a few days of completing 10 day course of axbx • Refer to ENT for tympanocentesis with culture ID
Chronic Suppurative OM • Persistance (>6 wks) of chronic inflammation of middle ear & mastoid in the presence of perforated or non-intact TM • +/- purulent ear discharge • Tx with meticulous cleaning and aspiration of external & middle ear, topical axbx ear drops, oral axbx • If this fails, then IV axbx with admission • Complications • Hearing loss, perforation or retraction pocket of TM, tympanosclerosis, adhesive OM, CSOM, cholesteatoma, mastoiditis, extradural abscess, subdural empyema, focal encephalitis, brain abscess, lateral sinus thrombosis, otic hydrocephalus
OM with effusion • Hearing loss is most prevalent complication • Tx to reduce risk of hearing loss • If occurs in young infants • Assoc with purulent URI • Permanent conductive or sensorineural hearing loss • Vertigo • Alterations in TM • Middle ear changes • Persistence of effusion for > 3 mos • Occurrence of episodes close together • Presence of craniofacial abnormalities • Impaired or deficient immunologic states
OM with effusion • Tx is observation or axbx • Surgical options like myringotomy or tympanostomy tubes; adenoidectomy
Otitis externa • Inflammatory condition of the auricle, external ear canal or outer surface of the TM • Causes: • Infection • Inflammatory dermatoses • Trauma • Most common orgs • Normal flora (Staph epi, Corynebacterium sp., alpha hemolytic strep) • P. aeruginosa • S. aureus • Fungi
Otitis externa • Clinical features • Itching or sense of fullness in ear • Pain, itching, edema, redness, tenderness of canal • Cheesy or purulent discharge • Pain with pressure on tragus or pulling up the auricle • TM will be red, thick & covered w/ flat vesicles • Disseminated infxn w/ tender, enlarged lymph nodes • If there is abscess, suspect S. aureus • If there is c/o intense itching, suspect Aspergillus niger (fungi) • Inspect for FB
Otitis externa • Treatment • Thorough & atraumatic cleaning of ear canal • Acetic acid eardrops (3-4x/d for 1 wk) • If canal edematous, place wick so drops can be passed in canal • Axbx drops • Cortisporin opthalmic suspension, • Ofloxacin (preferred for non-intact TM) • Ciprofloxacin with hydrocortisone • Oral axbx can be added if fail to respond w/in 48 h • Parenteral axbx in pts w/ progressive, unresponsive, sev. Infxn • Need cxs of canal secretions • No swimming while tx, encourage ear plugs even after tx
Pharyngitis • Infxn of pharynx & tonsils • Non-streptococcal • Most cases caused my viruses • Adenovirus • EBV • Influenza • Parainfluenza • Rhinovirus • HSV • Enterovirus • Sxs include sore throat & fever w/ cough, coryza, conjunctivitis or mucosal ulcerations
Pharyngitis • Non-streptococcal • Corynebacterium diphtheriae • Pseudomembrane can progress to airway obstruction, exotoxin that can cause myocarditis, cardiac dysrhythmias, neuritis w/ bulbar & peripheral paralysis, nephritis, hepatitis; tx w/ PCN or ERY & horse serum antitoxin • N. gonorrhoeae • If in young children, suspect abuse; throat cxs along w/ vaginal, rectal, urethral swabs & serum to test for hep B and syphillis; tx w/ ceftriaxone 125mg IM • EBV • Infectious mononucleosis; splenomegaly & hepatomegaly; malaise, fatigue, LAD & fever; serum for heterophil Ab • HIV type 1
Pharyngitis • Streptococcal • GABHS • Jan-May • Ages 4-11 yo; uncommon before age 3 • Sore throat & fever • Table 121-5 • RST, throat cx (mainstay of lab dx) • False neg. rate about 10% • Tx w/ PCN (no development of resistance even after decades of using) • PCN G 600,000u IM (if pt weighs <26 kg); 1.2 millionu (if > 26kg) • PEN VK or Amoxicillin oral • Table 121-6
Pharyngitis • Tx aimed at: • Preventing rheumatic fever • Preventing suppurative complications (PTA, cellulitis) • Hasten clinical recovery • Complications • Rheumatic fever • Post-streptococcal glomerulonephritis (not preventable w/ axbx; related to infxn w/ nephrogenic strains of strep) • Invasive GABHS (septicemia, TSS, pneumonia, cellulitis, lymphangitis, necrotizing fasciitis)