Download
1 / 14
160 likes | 395 Vues
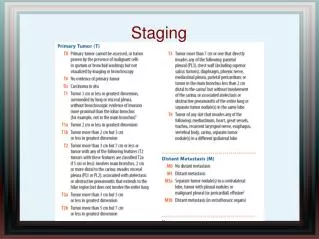
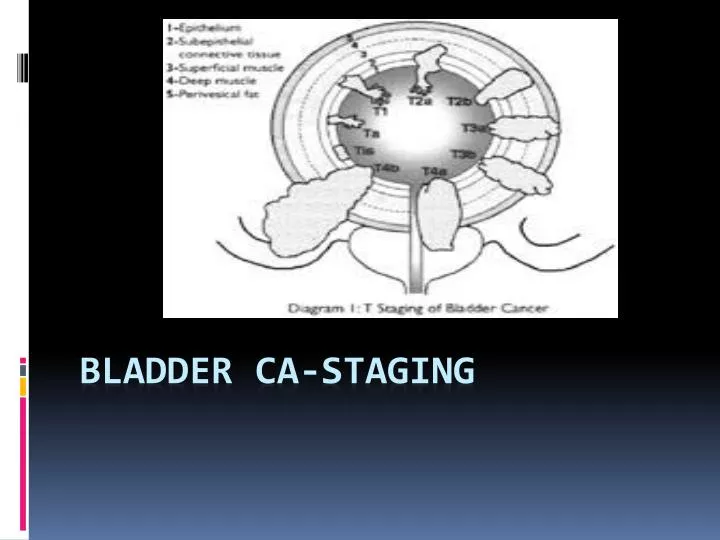
Bladder CA-Staging . a) and (b) Transaxial T2W1 of the bladder. The normal bladder muscle layer demonstrates low signal intensity (arrow), the mucosa intermediate signal (crossed arrow) with high signal urine within the bladder (B)

E N D
a) and (b) Transaxial T2W1 of the bladder. The normal bladder muscle layer demonstrates low signal intensity • (arrow), the mucosa intermediate signal (crossed arrow) with high signal urine within the bladder (B) • and intermediate signal perivesical fat (F). In (a), the normal high signal return from the seminal • vesicles (S) is seen. In (b), a more cranial section, the distal ureters (U) are seen as they enter the • bladder (B). The vas deferens (VD) is also clearly seen.
Transaxial T2W1 and (b) sagittal T2W1 through the bladder. These images demonstrate circumferential low • signal thickening of the bladder wall (arrows) in keeping with detrusor muscle hypertrophy due to • chronic bladder outlet obstruction
Sagittal T2W1 and (b) fat saturation contrast-enhanced T1W1 demonstrating an enhancing tumour invading • the superficial bladder muscle (arrows). The intact outer bladder wall is demonstrated (open arrow). • The patient has benign prostatic hypertrophy (asterisk). (Courtesy of Dr. M.Haider, Princess Margaret • Hospital, Toronto.)
Sagittal T2W1 through the bladder. There are multiple nodules of intermediate signal tumour involving the • superficial bladder muscle (arrows). These areas show an intact outer low signal bladder wall (crossed • arrows). Lying adjacent to this is abnormal intermediate signal that has extended across the full • thickness of the bladder wall (arrowheads) indicating T2b tumour. One of the focal areas of tumour • shows a deficit of the low signal bladder wall with intermediate signal extending across the whole • thickness of the bladder wall, with subtle extension into the perivesical tissues (open arrow), this area • is therefore radiologically a T3b tumour.
Transaxial T1W1 and (b) transaxial T2W1 of a male patient with transitional cell carcinoma (T) of the • bladder demonstrating transmural extension with stranding within the perivesical fat (arrows). There • are also multiple serpiginous structures (open arrows) in the perivesical fat immediately adjacent to the • tumour, which are of intermediate signal on T1 and high signal on T2. These are perivesical vessels • and could be confused with extra-vesicaltumour if only the T1W sequence was assessed. The filling • defect within the bladder represents benign prostatic hypertrophy (arrowheads
T2W1 demonstrating extension of tumour into the perivesical fat. Note the normal bladder wall • demonstrates low signal intensity (open arrows) while the tumour demonstrates intermediate-to-high • signal intensity (T), outlined by high signal urine and intermediate to high signal intensity perivesical • fat. The tumour is involving the right ureteric orifice and causing a right-sided hydroureter (U). Right • external iliac lymph node (N). Uterus (arrowhead). Rectum (R).
Sagittal T2W1. There is a large bladder tumour arising from the base of the bladder and extending along the • postero-superior bladder wall. The tumour is extending through the posterior bladder wall and • perivesical fat and is invading the vagina (arrows) and lower cervix (crossed arrow). Uterus (asterisk), • rectum (R), symphysis pubis (S).
T2W1 of the bladder. There is a large bladder tumour (T) extending to the rectus sheath anteriorly • (arrows). There is also tumour arising in the posterior bladder (asterisks) which is not invading muscle • (T2 or less) but is obstructing the left ureter(U)……….T4b
T3b N1 Bladder cancer. • Transaxial T2W1 of the bladder. There is a large intermediate signal tumour (T) involving the right anterolateral • bladder wall, extending into the perivesical fat. Multiple small perivesical nodes are seen • (arrowheads). These are noted to be of a similar signal intensity to the main bladder tumour. A right • internal iliac node (N) is seen with similar signal intensity to the tumour proper making it more likely • to be metastatic.
N2 Bladder cancer. • Transaxial T2W1 showing bilateral metastatic obturator nodes (N). The right obturator node measures between • 2.0 and 5.0 cm in greatest dimension, and has an irregular margin anteriorly (arrowheads) indicating • extra-capsular extension.
T3b N3 Bladder cancer. • Coronal T2W1 showing a large bladder tumour (T) extending into the perivesical fat. There is a right external • iliac node (N), >5.0 cm in longest dimension and of identical signal intensity to the primary tumour.
M1 Bladder cancer—bone metastasis. • Transaxial T1W1 through the pelvis showing an intermediate signal mass (M) In the body of the sacrum due to a • bone metastasis from the patient’s transitional cell bladder tumour.