Download
1 / 56
580 likes | 928 Vues
ESBL. Jasmin Fauteux March 29 th 2012. PLC Intake. 66 yo female with dysuria and pelvic pain Just returned from visit to Pakistan VS Normal Physical exam: Mild right CVA tenderness Seen 2d ago and given C ipro for UTI. UA: WBC-21-30 Nitrites +. E. Coli > 8 x 10 6.

E N D
ESBL JasminFauteux March 29th 2012
PLC Intake • 66 yo female with dysuria and pelvic pain • Just returned from visit to Pakistan • VS Normal • Physical exam: Mild right CVA tenderness • Seen 2d ago and given Cipro for UTI
UA: WBC-21-30 Nitrites +
E. Coli > 8 x 106 • Ampicillin R • Ceftriaxone R • Pip/tazo S • Cipro R • Nitrofurantoin S • TMP/SMX S Disposition?
Goals • Definition • Microbiology • Incidence • Risk factors • Morbidity • Management • Prevention
A new problem? • 1940s: First β-lactamase in E. coli • 1980s: Introduction of Cefotaxime in Europe • 1984: First reported case of ESBL in France and Germany • 1988: First case in US
Definitions • Beta-lactams • Beta-lactam ring that inhibits cell wall synthesis • Penicillins, cephalosporins, carbapenems and monobactams • Beta-lactamase • Bacterial enzymes that open the beta-lactam ring, inactivating the antibiotic • Currently over 600 β-lactamases
Extended spectrum β-lactamase • Activity against oxyimino-cephalosporins (3rd generation) and monobactams but not the cephamycins • Inhibition by beta-lactam inhibitors • AmpC • Resitant to cephamycins and beta-lactam inhibitors • Carbapenemase • Resistant to carbapenems
Extended spectrum β-lactamase • Heterogeneous group • Testing of various oxyimino-β-lactams required
Which bugs? • All Gram-negative bacterias • Klebsiella species • E. coli • Pseudomonas • Acinetobacter • Burkholderia • Citrobacter • Enterobacter • Morganella • Proteus • Salmonella • Serratia • Shigella
Detection • 2010 CLSI • New MIC criterias • Correlates with clinical outcome
Any gram-negative bacteria • Resistance to a single 3rd generation cephalosporin
12,8% 4,7% 33,8% 32,4% 26,6% 13,9% 35,5% 26,3% 54,9% 12,9% 45,5% 25,9% Klebsiella E. Coli
Canada CANWARD 2008 *CANWARD 2007-2009
Calgary E. coli Molecular Epidemiology over an 11-Year Period (2000 to 2010) of Extended-Spectrum -Lactamase-ProducingEscherichia coli CausingBacteremiain a Centralized Canadian Region, Peirano et al, Journal of Clinicalmicrobiology
Calgary E. Coli • 2008-2010 Antibiograms • Sensitivity to Ceftriaxone
Calgary K. pneumoniae Molecularepidemiology of extended-spectrum-b-lactamase-producingKlebsiellapneumoniae over a 10 year period in Calgary, Canada, Peirano, G. Journal of Clinical Microbiology
Calgary Klebsiella • 2008-2010 Antibiograms • Sensitivity to Ceftriaxone
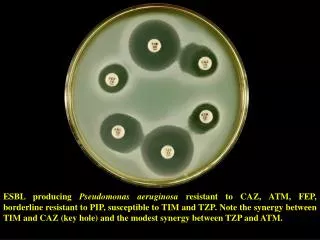
Calgary P. aeruginosa • 2008-2010 Antibiograms
Risk Factors
Carrier -24-33% still colonized at 6mo -10-12% still colonized at 3+ years
All antibiotics • 3rd generation cephalosporins • Restriction of use caused reduction in ESBL infection
88% of healthy travelers returning from India were colonized with ESBL E.coli
12,8% 4,7% 33,8% 32,4% 26,6% 13,9% 35,5% 26,3% 54,9% 12,9% 45,5% 25,9% Klebsiella E. Coli
- Hospital stay and contact- Health care workers contact- Long term care
Instrumentation • Central or arterial line • Urinary catheter • Mechanical ventilation • G/J-tube • Hemodialysis
Severity of illness • Comorbidities • Low birth weight (NICU)
Hospital cost and length of stay roughly double
-OR for mortality = 2,35 -Adjusted for sepsis severity and with appropriate initial therapy = 1,37
Management • High bacterial inoculum • Uncomplicated UTI
Everything but uncomplicated UTI • Carbapenems • Need to speak to ID • Ertapenem 1g IV q 24hrs • In patient vs outpatient
Serious bacterial infectionsTreatment • Even with In Vitro susceptibility, we should not use: • 3rd generation cephalosporins • 4th generation cephalosporins* • Cephamycins • Pip/tazo • Fluoroquinolones • Aminoglycosides * Might change with 2010 CLSI, potential future therapy
What if… Speak to ID -Amikacin -Tigecycline -Colistin
Uncomplicated UTI • If sensitive -Nitrofurantoin - 5 days -Fosfomycin* - 3g PO once -Fluroquinolones – May be considered *Not available in Canada
Prevention • Isolation of ESBL • Responsible antibiotic use • Avoiding unnecessary procedures
Contact Isolation • Reduces incidence of ESBL by 55% • In Calgary: - no isolation - no screening
Antibiotic stewardship • Use of narrower spectrum antibiotics • Avoiding cephalosporins and fluroquinolones • Minimizing days of therapy
Carbapenem resistance • Pseudomonas: 3,3% • A. Baumannii: 2,7% • E. Coli & Klebsiella: 0,1% • Mortality:40-60% • Contact ID & contact isolation