Download
1 / 15
150 likes | 153 Vues
Learn about the difference between Transformation of Care, PCMH, and Change Concepts in healthcare transformation. Discover the key elements of Patient-Centered Medical Home (PCMH) and the eight Change Concepts for PCMH. Explore the actions and strategies for better access, continuity, coordinated care, and value-based reimbursement.

E N D
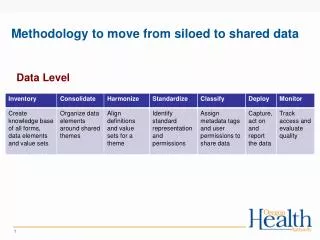
The Basics on GCACH Alignment from Siloed Projects to Transformation of Care August 3, 2018
The Care Transformation Alphabet: What's the difference between Transformation of Care, PCMH and Change Concepts?
Healthcare Transformation Healthcare transformation is the effort to reorient the entire delivery system around the user of the industry’s services: the patient.
Patient-Centered Medical Home (PCMH) • Also referred to as . . . • The primary care medical home • Advanced primary care • The healthcare home • The PCMH is a redesigned approach to primary care that views a strengthened, long-term relationship between patient and primary care team as central to better care.
Patient-Centered Medical Home (PCMH) • Research identifies six fundamental elements that define a primary care practice as operating as a medical home: • A care team that extends beyond the primary care physician (PCP) • Disease registry utilization • Comprehensive care delivery that involves necessary preventive care and chronic disease management • Active patient engagement • Improved patient access • Cross-continuum care coordination
Change Concept • Eight Change Concepts for PCMH • Engaged leadership • Quality improvement strategy • Empanelment • Continuous, team-based healing relationships • Organized, evidence-based care • Patient-centered interactions • Enhanced access • Care coordination
Defining Actions Access and Continuity: Because health care needs and emergencies are not restricted to office operating hours, primary care practices optimize 24/7 access to care guided by the medical record. Planned Care for Chronic Conditions and Preventive Care: Participating primary care practices proactively assess their patients to determine their needs and provide appropriate and timely chronic and preventive care. Risk-Stratified Care Management: Patients with serious or multiple medical conditions need extra support to ensure they are getting the medical care and/or medications they need. Coordination of Care Across the Medical Neighborhood: Practices work closely with patients’ health care providers, coordinating and managing care transitions, referrals, and information exchange.
Assess and Align In any medical setting, whether you are assessed using the Patient-Centered Medical Home Assessment (PCMH-A) or The Maine Health Access Foundation Assessment (MeHAF) the Practice Transformation approaches contribute to overall better patient care and improved success in value-based reporting and reimbursement.
Value-Based Care • Value-based care • Alternative to fee-for-service reimbursement • Primary features • Ties payments for care delivery to the quality of care provided • Rewards providers for both efficiency and effectiveness
Value-Based Care • Value-based care models center on • Patient outcomes • How well healthcare providers improve quality of care based on specific measures such as . . . • Reducing hospital readmissions • Using certified health IT • Improving preventative care
Consistency • The most common measures in VBR contracts remain the same year to year • Follow-up after hospitalization • Emergency room use • Readmission rates • For most provider organization executives, these constitute the “must have” organizational performance measures if you’re interested in building partnerships with health plans. https://www.openminds.com/market-intelligence/executive-briefings/value-based-reimbursement-numbers/
Top 3 Needs for VBR Sustainability More and better data management and reporting for managing VBR contracts A technology infrastructure that supports VBR Management talent with the expertise to use that data to manage care
“The goal is straightforward but ambitious: Replace the nation’s reliance on fragmented, fee-for-service care with comprehensive, coordinated care using payment models that hold organizations accountable for cost control and quality gains.” https://revcycleintelligence.com/features/what-is-value-based-care-what-it-means-for-providers Sustainability: shared savings and maximizing reimbursement
Any Questions? Please feel free to contact: Samantha Werdel Swerdel@gcach.org Jenna Shelton Jshelton@gcach.org Martin Sanchez Msanchez@gcach.org