Download
1 / 52
520 likes | 602 Vues
Sexually Transmitted Infections, Including HIV: Impact on Women’s Reproductive Health. Catherine Ingram Fogel, PhD, RN, FAAN Beth Perry Black, PhD, RN. Introduction . Sexually transmitted infections (STIs) affect approximately 19 million Americans every year.

E N D
Sexually Transmitted Infections, Including HIV: Impact on Women’s Reproductive Health Catherine Ingram Fogel, PhD, RN, FAAN Beth Perry Black, PhD, RN
Introduction Sexually transmitted infections (STIs) affect approximately 19million Americans every year. They account for 87 percent of the top 10 most frequently reported diseases (Cates, 1999). One in 4 Americans will contract an STI during their lifetime (Gonen, 1999).
Introduction (Continued) The nurse’s role in promoting women’s reproductive and sexual health: Counsel women about STI risk Encourage risk-reduction measures Provide education about STI prevention Be knowledgeable about treatment and management strategies
Reproductive Health Concerns Passing an STI to a fetus or newborn Potentially life-threatening health conditions Damage to the brain, spinal cord, eyes and auditory nerves Spontaneous abortion Stillbirth Premature rupture of membranes (PROM) Low birthweight (LBW) Preterm delivery
STI Transmission: Biological Factors Women are more likely to become infected with STIs than men. More than 50 percent of bacterial and 90 percent of viral STIs are asymptomatic and likely to be undetected in women (CDC, 2006a, Futterman, 2001). Young women are more susceptible than premenopausal women to HIV and cervical infections (Varney et al., 2004).
STI Transmission: Social Factors Poverty Lack of education Social inequity Inadequate access to health care Gender-power imbalances Cultural proscriptions
STI Transmission: Other Factors Alcohol use Drug use Depression Sexual abuse
Activities critical to STI prevention and control: Educating those at risk Vaccinating pre-exposure Detecting untreated cases Effectively diagnosing, treating and counseling Assessing, treating and counseling sex partners STI Prevention (CDC, 2006b)
STI Prevention (Continued) Nurses should: Provide individual prevention counseling. Encourage safer sex practices. Suggest strategies to enhance condom negotiation skills. Educate women about dual protection for STI and pregnancy prevention.
Safer Sex Practices Use barrierprotection. Find out about a sex partner’s past sexual behavior and STI exposure. Avoid partners who have had multiple sex partners. Reduce the number of sex partners. Engage in low-risk sex practices. Avoid the exchange of body fluids. Avoid sexual contact with casual acquaintances.
Caring for a Woman with an STI Counseling is essential to: Prevent new infections or reinfection Increase treatment compliance Provide support during treatment Assist a woman in discussion with her partner
Caring for a Woman with an STI(Continued) Nurses are legally responsible for reporting reportable diseases and must know state reporting requirements. Chlamydia is reportable in most states. Gonorrhea, syphilis, HIV and AIDS are reportable in all states. Nurses must inform the woman when an STI will be reported.
Cervicitis: Chlamydia The most common and fastest spreading STI in American women (CDC, 2002d, 2006b). Up to 80 percent of infections are asymptomatic (Faro, 2001). Prevalence in pregnancy ranges between 2 percent and 21 percent (Faro, 2001).
Pregnancy complications: PID Postpartum or postabortion endometritis and salpingitis Preterm delivery PROM Stillbirth Neonatal complications: Acquires infection from mother Infections to the mucous membranes of the eye, oropharynx, urogenital tract and rectum LBW Ophthalmia neonatorum Chlamydia: Pregnancy and Newborns
Cervicitis: Gonorrhea An estimated 1 million Americans contract gonorrhea each year (CDC, 2002e). Most infected individuals are 20 years old or younger (CDC, 2002e).
Pregnancy complications: Chorioamnionitis Intrauterine growth restriction (IUGR) Pelvic abscess or Bartholin’s abscess PID Postpartum sepsis Preterm delivery PROM Spontaneous septic abortion Neonatal complications: Acquires infection from mother Ophthalmia neonatorum Sepsis Gonorrhea: Pregnancy and Newborns
Pelvic Inflammatory Disease (PID) Caused by a variety of infectious agents. Results from the ascending spread of microorganisms from the vagina and endocervix to the upper genital tract. More than 1 million women in the U.S. experience an episode of PID every year; at least 25 percent of these women experience long-term sequelae (CDC, 2006b). Teenagers have the highest risk.
Pregnancy complications: Ectopic pregnancy Fetal wastage Infertility Inflammatory disorders of the upper genital tract Maternal morbidity Preterm delivery Neonatal complications: Acquires infection from mother Death PID: Pregnancy and Newborns
Ulcerative Genital Infection: Syphilis An estimated 40,000 cases of primary and secondary syphilis in the U.S. each year(ASHA, 2005). Rates are 16 times higher for African- Americans than for White Americans(ASHA, 2005). Other STIs affect mostly teens and young adults; syphilis persists into the early 30s.
Pregnancy complications: Preterm labor Spontaneous abortion Stillbirth Neonatal complications:(March of Dimes, 2005): Acquires infection from mother Blindness Bone and tooth abnormalities Brain damage Hearing loss Death Syphilis: Pregnancy and Newborns
Ulcerative Genital Infection: Genital Herpes Simplex Virus (HSV) Affects an estimated 50 million Americans. Initial infection lasts about 3 weeks. Pregnant women with an active, visible lesion should be screened. If lesions or prodromes are not present at onset of labor, vaginal delivery is acceptable.
HSV: Pregnancy and Newborns Maternal complication: Cesarean delivery if there are prodromes or active lesions when the woman goes into labor Neonatal complications: Acquires infection from mother; rates are highest when herpes is acquired near time of delivery Eye infections Severe disseminated or CNS infection resulting in mental retardation or death
Ulcerative Genital Infection: Chancroid Appears mostly in urban areas. Is a cofactor for HIV infection. An abrasion is necessary for the organism to penetrate the skin. Neonates can acquire the infection from the mother.
Diseases Characterized by Vaginal Discharge Vaginal discharge and itching are among the most frequent reasons a woman seeks help from a health care provider. Vaginal discharge resulting from infection must be distinguished from normal secretions.
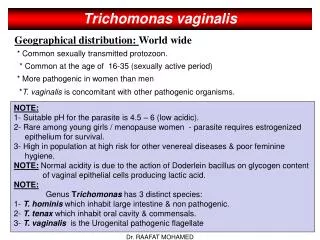
Diseases Characterized by Vaginal Discharge: Trichomoniasis Affects approximately 3 million women annually (Gorroll, 2001; Hatcher, et al., 2004) Pregnancy complications: Preterm delivery PROM Neonatal complications: Acquires infection from mother LBW
Diseases Characterized by Vaginal Discharge: Bacterial Vaginosis (BV) The most common type of abnormal vaginal discharge in childbearing women(Calzolari et al., 2000; Varney et al., 2004)
Pregnancy complications: Chorioamnionitis Miscarriage Postpartum endometritis Preterm labor and delivery PROM Neonatal complications: Acquires infection from mother Infections LBW BV: Pregnancy and Newborns (CDC, 2006b; Koumans et al., 2002)
Vaginal Discharge: Vulvovaginal Candidiasis (VVC) VVC, or yeast infection, is the second most common type of vaginal infection in the U.S. (CDC, 2002e). The most common symptoms are vulvar and vaginal pruritus. Discharge is often thick, white, curdy and cottage-cheese-like.
Human Papillomavirus (HPV) The most prevalent viral STI in the U.S. (Hatcher, 2004; Schaffer, 2003) One million new infections yearly (CDC, 2001). Most are asymptomatic, subclinical or unrecognized (Hawkins, Roberts-Nichols & Stanley-Haney, 2000). More frequent in pregnant than non-pregnant women (CDC, 2001).
HPV: Pregnancy and Newborns Pregnancy complications: Cesarean delivery Neonatal complications: Acquires infection from mother Juvenile laryngeal papillomata (JLP)
Hepatitis A (HAV) The most common form of hepatitis Acquired through a fecal-oral route No perinatal transmission (Sinclair, 2004) Pregnancy complications: Spontaneous abortion and preterm labor due to dehydration, fever and hypovolemia Neonatal complication: LBW
Hepatitis B (HBV) Transmitted through infectious blood or body fluids. Is approximately 100 times more infectious than HIV (CDC, 2003). Neonatal complications: Acquires infection from mother Life-long carrier Liver disease and liver cancer
Hepatitis C (HCV) HCV is the most common chronic blood-borne infection in the U.S. An estimated 2.7 million persons are chronically infected (CDC, 2006b).
HCV: Pregnancy and Newborns Neonatal complications: 5 of every 100 infants exposed become infected, most often during or near delivery (CDC, 2006b). Breastfeeding does not seem to transmit HCV; however, HCV-positive mothers should consider not breastfeeding if their nipples are cracked or bleeding.
Human Immunodeficiency Virus (HIV) An estimated 17.6 million women worldwide are living with HIV/AIDS (CDC, 2002a; NIAID, 2006). For many, HIV is treated as a chronic infection, and it may never progress to AIDS (Varney et al., 2004). The clinical goal is to minimize viral replication.
Effects of HIV on the Immune System HIV is a retrovirus that targets CD4+ T-cells, depleting the number of cells and impairing cell function. Unimpeded, HIV can destroy up to 1 billion CD4 cells per day. HIV is genetically highly variable, mutating with apparent ease.
HIV Complications Pregnancy complications: Gradual loss of immune function Inability to fight disease Increased susceptibility to infections, certain cancers and other life-threatening problems Neonatal complications: Acquires infection from mother Gradual loss of immune function
HIV/AIDS Epidemiology AIDS is the fifth leading cause of death among women ages 25 to 44 in the U.S., and the third leading cause of death in Black women in this age group (CDC, 2002a,2007b). Seventy-nine percent of women with AIDS in the U.S. are African-American or Hispanic (CDC, 2007b; NIAID, 2006).
HIV Testing: Pregnant Women Include HIV testing in routine prenatal screening. Screen after the woman is informed that testing will be done, unless she declines (CDC, 2006b; 2006c). Separate consent for HIV test is not required. Repeat screening in the third trimester for women at high risk or those living in areas with elevated rates of HIV infection in pregnant women. Provide oral and written information to women.
Posttest Counseling: The Seropositive Woman Most HIV+ women are diagnosed during childbearing years (CDC, 2002e; 2002f; 2006c). Making the decision to become pregnant or forego future childbearing should occur only after the woman is fully informed about HIV and pregnancy. The antiretroviral zidovudine (ZDV) given in pregnancy has reduced perinatal transmission to low levels.
Posttest Counseling: The Seronegative Woman Seronegative women should receive counseling and education about behavior change to reduce the risk of contracting HIV. If indicated, serial testing should be encouraged.
Modes of HIV Exposure (Jacobson & Hicks, 2000) HIV is transmitted through: Sexual contact with vaginal and cervical secretions and semen Infected blood, blood components and clotting factors Vertical transmission to the fetus or to the infant through breastfeeding
HIV in Pregnancy The baseline rate of perinatal HIV transmission without prophylactic therapy is approximately 25 percent (Anderson, 2001). Perinatal transmission rates drop to <2 percent with prophylactic administration of antiretroviral drugs ZDV and AZT, scheduled cesarean section delivery and avoidance of breastfeeding (CDC, 2006b).
HIV in Pregnancy (Continued) Cesarean delivery is recommended as an intervention to prevent perinatal HIV transmission only during the active stages of HIV in untreated women (Public Health Service Task Force, 2002). When replacement feeding is possible, HIV+ mothers should avoid breastfeeding (WHO et al., 2003).
HIV Treatment Resource For free, 24-hour clinical advice for treating HIV-infected pregnant women and their infants, call: The National Perinatal HIV Consultation and Referral Service 1-888-448-8765
Antiretroviral Therapy (ART) Effective ART uses a combination of antiretroviral therapies (cART) that slow viral replication. Providers should offer cART to all women who show signs of HIV disease progression or AIDS-defining criteria.
Antiretroviral Therapy (Continued) Eleven anti-HIV drugs are approved for use with pregnant women (Perinatal HIV Guidelines Working Group, 2006). These include: Nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs) Protease inhibitors (PIs)
Adherence to ART A critical nursing challenge is to teach and counsel HIV+ women to adhere to their prescribed regimen. Failure to adhere results in: Rapid increase in viral load Concurrent immune-system damage Risk of developing a resistant strain
Prevention of Opportunistic Infections A single dose of double-strength trimethoprim-sulfamethoxazole (Septra, Bactrim) reduces the incidence of pneumocystis carinii pneumonia (PCP), toxoplasmosis and bacterial infections (CDC, 1999b). It can be used by pregnant women when the risk of infection outweighs the risk of the medication.
Prevention of Opportunistic Infections(Continued) Nurses should counsel HIV+ women: To practice basic hygiene To eat healthy foods To exercise To avoid smoking, drinking alcohol and using illegal drugs To reduce their stress To reconsider foreign travel