Download
1 / 70
1.34k likes | 4.27k Vues
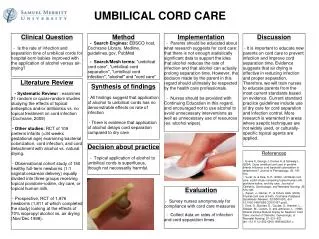
Lecture 17 ABNORMALITIES OF PLACENTA AND UMBILICAL CORD. Prof. Vlad TICA, MD, PhD. PLACENTA: PHYSIOLOGY AND FUNCTION. Fetus entirely dependent on placenta until birth Maternal and fetal blood kept separate by placental barrier Protects the infant from infection and harmful substances

E N D
Lecture 17 ABNORMALITIES OF PLACENTA AND UMBILICAL CORD Prof. Vlad TICA, MD, PhD
PLACENTA: PHYSIOLOGY AND FUNCTION Fetus entirely dependent on placenta until birth Maternal and fetal blood kept separate by placental barrier Protects the infant from infection and harmful substances Acts as endocrine organ - makes hormones to maintain pregnancy Made of 12-20 cotyledons
PLACENTA: PHYSIOLOGY AND FUNCTION Fetal blood transported to placenta via 2 umbilical arteries Umbilical arteries get smaller and become arterioles then villi Villi suspended in pools of maternal blood in the lacunae Fetal blood returns to fetus via umbilical vein
ABRUPTIO PLACENTAE 1. DEFINITION • Separation of the normally situated placenta from its uterine site of implantation after 20 weeks gestation, but before delivery of the placenta
ABRUPTIO PLACENTAE 2. PLACENTAL GRADES Grade 0 - Patient asymptomatic. Small retroperitoneal clot seen after delivery Grade 1 - Vaginal bleeding, may have abdominal tenderness or slight uterine tetany, mom and baby not in distress Grade 2 - Uterine tenderness, tetany with / without evidence of bleeding, baby shows signs of distress Grade 3 - Uterine tetany, severe bleeding may not be visible. Baby is dead. Mom often has coagulopathy
ABRUPTIO PLACENTAE 3. INCIDENCE Varies from 1/55 to 1/250 cases Incidence greater with increasing parity or history of abruption
ABRUPTIO PLACENTAE 4. ETIOLOGY Unknown Possibly begins with degenerative changes in the small arterioles that supply the intervillous spaces, resulting in thrombosis, degeneration of the decidua, and finally rupture of the vessel Then tearing and bleeding in the inner layer of the endometrium and decidua basalis Hematoma forms along with retroperitoneal clot, compresses adjacent placenta, causing local destruction Further bleeding causes increased pressure behind the placenta which causes further separation
ABRUPTIO PLACENTAE 5. CONDITIONS ASSOCIATED WITH ABRUPTION: Hypertension - 5x higher Trauma Short umbilical cord Polyhydramnios IV cocaine use Uterine anomalies
ABRUPTIO PLACENTAE 5. CONDITIONS ASSOCIATED WITH ABRUPTION: OB history: 1. History of spontaneous abortions 2. Premature labor 3. Antepartum hemorrhage 4. Stillbirth / neonatal death 5. Parity > 7 - 6x greater 6. History of abruption - 30x greater 7. Cigarette smoking - decidual necrosis
ABRUPTIO PLACENTAE 6. SIGNS AND SYMPTOMS • Depends on type of abruption: • Mild c/o labor pains, may only have slight uterine irritability • May have no / only small amount of bleeding • Severe knife-like pain with board-like abdomen • May / may not see bleeding • Uterus could be tender at point of separation or may be generalized over entire abdomen
ABRUPTIO PLACENTAE 6. SIGNS AND SYMPTOMS • Depends on type of abruption: • Increased uterine distention - elevated fundal height • Bleeding may be minimal or diffuse. Can be port-wine, dark, or bright red • Symptoms are determined by amount of blood lost • Shock is severe • Fetal distress or death
ABRUPTIO PLACENTAE 7. DIAGNOSIS Based on hystory, physical exam, lab values NO analgesia / anesthesia until diagnosis confirmed Vaginal bleeding with / without pain Increased uterine tone, tenderness Shock Fetal distress U/S for placental localization, position Palpation of abdomen, measure fundal height Confirm after delivery-inspect placenta
ABRUPTIO PLACENTAE 8. MATERNAL/ FETAL OUTCOME Mortality rate < 1%; if undetected until fetal death, mortality rate is 10% DIC - 30% Renal failure from hypovolemia Amniotic fluid embolus Uterine rupture Postpartum endometritis Postpartum hemorrhage
ABRUPTIO PLACENTAE 9. MEDICAL MANAGEMENT US to R/O placenta praevia Bedrest (lateral position) IV with large bore catheter Type and crossmatch, CBC, platelet count, fibrinogen, bleeding time Frequent vital signs Assess for signs of shock - cold, clammy skin, pale, anxious, thirsty Assess FHR and uterine activity
ABRUPTIO PLACENTAE 9. MEDICAL MANAGEMENT Mark top of fundus (check to see if rising) Observe for signs of vaginal bleeding C/S for fetal distress, maternal blood loss or compromise, coagulopathy, poor labor progress Strict I & O Amniotomy to assess blood in fluid Oxygen per mask Avoid episiotomy Be aware of postpartum hemorrhage
PLACENTA PRAEVIA 1. DEFINITION Abnormally implanted placenta placed totally / partially in the lower segment of the uterus, rather than in the fundus When the cervix begins to dilate and efface the placenta separates, allowing bleeding form the open vessels
PLACENTA PRAEVIA 2. CLASSIFICATION Complete - internal os is completely covered by the placenta Partial - a portion of the cervical os is covered by the placenta Marginal - The edge of the placenta extends to the edge of the cervical os
PLACENTA PRAEVIA 3. INCIDENCE • Depends on which trimester pregnancy is in: • 2nd trimester - 45 % in lower uterine segment • 3rd trimester - 0.5 to 1 % in lower uterine segment • Occurs more often in multiparas - 80 % • History of praevia - 12x more likely • More common with history of abortions • C/S, molar pregnancies, fibroids, uterine surgery
PLACENTA PRAEVIA 4. ETIOLOGY • Unknown cause • It is thought that when the embryo is ready to implant and the decidua in the fundus is deficient, it will choose another spot lower in the uterine segment • Placentas are larger on the maternal side, cord often has marginal or vellamentous insertion • Suggests that the placenta was growing toward more favorable decidua
PLACENTA PRAEVIA 4. ETIOLOGY Endometriosis after previous pregnancy Uterine scars - abortions, C/S, molar pregnancy Tumors altering contour of uterus Close pregnancy spacing Multiparity Large placenta - in multiple gestations or erythroblastosis fetalis High altitudes Male fetus
PLACENTA PRAEVIA 5. DIAGNOSIS Painless bright red vaginal bleeding - usually 1st bleeding episode not before 30 weeks Sometimes suspected with oblique / transverse lie Diagnosed by U/S 80-90% - bleeding occurs without warning Uterus non-tender - no rise in fundal height Often occurs when sleeping 1st episode usually scant, each episode more Shock May deliver by C/S, if placenta covers cervix
PLACENTA PRAEVIA 6. MATERNAL AND FETAL OUTCOME Mortality < 1%, morbidity = 20% Most will have at least one significant hemorrhage, 25% will go into shock Vaginal and cervical lacerations occur more often with vaginal delivery Poor endometrium may contribute to placenta accreta Fetal mortality 20% - prematurity, hypoxia, developmental disorders
PLACENTA PRAEVIA 7. MEDICAL MANAGEMENT • Depends on gestational age and severity of bleed: • Strict bedrest • IV - large bore catheter (16 gauge) • CBC, type & screen, platelet count, fibrinogen, bleeding time • If HCT < 30% → transfuse • No pelvic exams • Adequate hydration, accurate I & O
PLACENTA PRAEVIA 7. MEDICAL MANAGEMENT • Tocolysis for contractions • No douching or intercourse • Oxygen per mask • Serial U/S to check for placental placement, fluid level, fetal growth • C/S for large blood loss
PLACENTA ACCRETA 1. DEFINITION a rare condition all or part of placenta adherent to the myometrium the normal spongy layer of decidua is absent / defective, therefore placental villi grows down through the endometrium into the myometrium
PLACENTA ACCRETA 2. TYPES • Accreta - villi extends too far into endometrium • Increta - villi invade into myometrium • Percreta - villi invade through myometrium to the serosa layer
PLACENTA ACCRETA 3. INCIDENCE 1 / 7000
PLACENTA ACCRETA 4. PREDISPOSING FACTORS Implantation over a previous C/S scar / other surgical scar in the uterine cavity Previous curretagge Prior history of endometritis / other endometrial trauma High parity Placenta previa sometimes precludes accreta
PLACENTA ACCRETA 5. SIGNS AND SYMPTOMS • None until delivery • Depends on depth, site of penetration, number of cotyledons involved • Partial accreta - some cotyledons may separate from the uterine wall, leaving open, bleeding vessels • The uterus is unable to contract because of the adherent placenta still within the uterine cavity • Profuse hemorrhage • Total accreta - tearing occurs when doctor tries to deliver placenta • Uterine inversion may occur
PLACENTA ACCRETA 6. DIAGNOSIS Attempts to remove placenta reveals placental adherence
PLACENTA ACCRETA 7. OUTCOME Hemorrhage Shock Uterine inversion Hysterectomy
PLACENTA ACCRETA 8. TREATMENT Large bore IV catheter IV fluids, blood US Type and screen, CBC, platelet count, fibrinogen, bleeding time Accurate I & O Assess vital signs D & C / hysterectomy
MULTILOBED PLACENTA BILOBED OR PLACENTA BILOBATA • Incidence: 2-8% of placentas • Roughly equal size lobes are separated by a segment membranes • Umbilical cord may insert in either of the lobes or in velamentous fashion or in between the lobes
MULTILOBED PLACENTA PATHOGENESIS • Arise due to implantation in areas of decrease uterine perfusion • Example: • Lateral implantation in between anterior and posterior walls of the uterus with one lobe on the other and one on the posterior wall
MULTILOBED PLACENTA PATHOGENESIS • Other local factors leading to multilobulation: • Implantation over leiomyomas • Area of previous surgeries • In the cornu • Over the cervical os
CIRCUMVALLATE PLACENTA The fetal surface of the placenta is exposed thorough a ring of chorion and amnion opening around the umbilical cord
SUCCENTURIATE PLACENTA One or more accessory lobes of the villi have developed Vessels from the major to the minor lobes are only supported by membrane This increases the likelihood that the minor lobe(s) are may be retained during the third stage of labor