Download
1 / 50
530 likes | 959 Vues
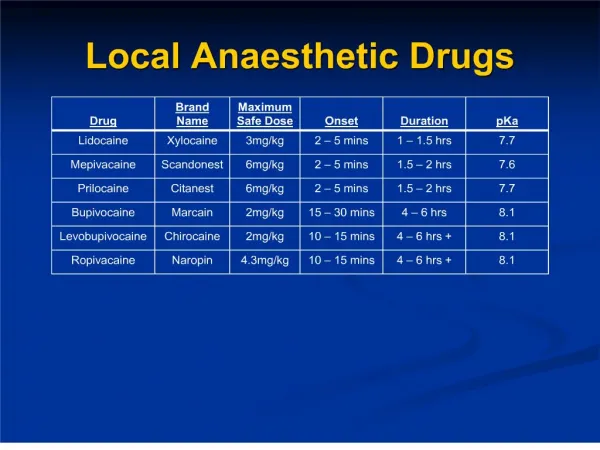
LOCAL ANAESTHETIC - Technique EO 006.01. UNCLASSIFIED//REL TO NATO/ISAF. Lesson Plan Overview. Technique Overview Infiltration Technique Inferior Alveolar Nerve (IAN) Block Technique Long Buccal Nerve Injection Periodontal Ligament Injection . Technique Overview.

E N D
LOCAL ANAESTHETIC - Technique EO 006.01 UNCLASSIFIED//REL TO NATO/ISAF
Lesson Plan Overview • Technique Overview • Infiltration Technique • Inferior Alveolar Nerve (IAN) Block Technique • Long Buccal Nerve Injection • Periodontal Ligament Injection
Technique Overview • Assemble armamentarium • Select appropriate technique and agent • Inspect cartridge • Review patient medical history • Prepare the patient • Apply topical anaesthetic
Technique Overview • Establish a firm hand rest • Make tissue taut • Landmark injection site • Orient bevel • Direct needle to desired location • Insert needle • Slowly advance the needle
Technique Overview • Stop at desired site • ASPIRATE • Slowly inject • Communicate with patient • Slowly withdraw needle • Recap SAFELY • Observe patient and assess anaesthesia
Technique Overview 1. Assemble Armamentarium • Syringe • Cotton tip applicator • Short needle • Long needle • Cartridge of local anaesthetic • Gauze • Mirror • Explorer • Safety capping device (optional)
Technique Overview 2. Select appropriate technique and agent • Consider location • Presence of infection • How many teeth • What procedure 3. Inspect cartridge – some things to consider • Expiration date • Solution • Damaged cartridge
Technique Overview 4. Review patient medical history: • Look for contraindications – eg allergy to amide local anaesthetic (rare) • Look for systemic problems – high blood pressure, recent heart attack, etc. 5. Prepare the patient • Tell patient what you are doing • Make sure patient has bib and safety glasses • Position patient as required for procedure
Technique Overview 6. Apply topical anaesthetic • Pull tissue taut • Dry injection site with gauze • Apply cotton applicator with small amount of topical for at least 1 minute 7. Establish firm hand position • Make sure your hand has at least one point of contact • Two is better
Technique Overview 8.Make tissue taut 9. Landmark injection site • Inferior Alveolar Nerve Block • Infiltration • Periodontal Ligament Injection 10. Orient bevel • Important for infiltration and PDL injection 11. Direct needle to desired location • Mental image of where you want the tip to end
Technique Overview 12. Insert Needle 13. Slowly advance the needle 14. Stop desired site • For infiltrate = root apex • For IAN Block = bone • PDL = resistance
Technique Overview 15. ASPIRATE • What is aspiration? • For the nerve block, always aspirate (pull in) to ensure your needle is not inside the artery • If it is inside, the blood will come into the cartridge • If not, the needle is in the right place
Technique Overview 16. Inject slowly • Decreases pain • Decreases risk of intravascular 17. Communicate with patient 18. Slowly withdraw needle 19. RECAP SAFELY 20. Observe patient and assess anaesthesia • Watch for allergic reaction, syncopy, other adverse signs • Anaethesia can take up to 10 minutes or more for a block
LOCALINFILTRATION • Teeth are anaesthetized by injecting close to the target tooth • The needle is inserted through the mucosa, next to the target tooth, to a estimated depth near the tooth root apex • Local Infiltration • Teeth are anaesthetized by injecting close to the target tooth • The needle is inserted through the mucosa, next to the target tooth, to a estimated depth near the tooth root apex.
LOCALINFILTRATION • The anesthetic diffuses through: • Local Infiltration • The anesthetic diffuses through: • 1.Periosteum (thin tissue covering of bone) • 2.Outer Cortical Plate (hard bone) • 3. Inner Cancellous Bone (soft bone) • 4. Alveolar Bone • 5. Periodontal Ligament • 1.Periosteum (thin tissue covering of bone) • 2.Outer Cortical Plate (hard bone) • 3. Inner Cancellous Bone (soft bone) • 4. Alveolar Bone • 5. Periodontal Ligament
LOCALINFILTRATION Point of Insertion • It may be found with ease by pulling the lip or cheek slightly away from the teeth as well as downward in the case of the upper jaw or upward in the case of the lower jaw. • The bevel of the needle should be facing the bone. AFAMS Dental Advisor Team
LOCALINFILTRATION • Puncture the tissue by pressing the needle tip against the tissue at this fold • At the same time the tissue is pulled over the needlepoint just as the puncture is made. A drop of anaesthetic is deposited in the tissue. • mlp AFAMS Dental Advisor Team
LOCALINFILTRATION • The needle is then advanced slowly toward the root apex in line with the long axis of the tooth. • Anaesthetic is slowly deposited as the needle is advanced. AFAMS Dental Advisor Team
LOCALINFILTRATION • The final resting point of the end of the needle should be slightly distal to the apex of the root. • The syringe should then be aspirated to make sure no blood vessels have been entered. • Then inject the rest of the anaesthetic. AFAMS Dental Advisor Team
LOCALINFILTRATION • The injection should be made very slowly. All anaesthetic should be given. • Rapid injections will likely result in pain, swelling and poor anaesthesia. AFAMS Dental Advisor Team
LOCALINFILTRATION Waiting Time • It may take 5 minutes to anaesthetize lower teeth and about 3 minutes in the case of upper teeth. • The gingiva area to be operated upon should be tested by puncturing it with the tip of an explorer in order to insure that it is properly anaesthetized. • The patient may sense pressure, but there should be no pain. AFAMS Dental Advisor Team
LONG BUCCAL NERVE INJECTION Waiting Time • Results are not as reliable in the lower molar region if the long buccal injection is not done. • The Long Buccal Nerve supplies sensation to the mandibular molar buccalgingiva and mucosa. AFAMS Dental Advisor Team
TECHNIQUES OF ANAESTHESIA FOR MAXILLARY General Considerations • Maxilla has very porous bone, with the exception of the zygomatic processes superior to the maxillary first molars. • Anaesthetic will diffuse through it, therefore local infiltrations are adequate for operative work. AFAMS Dental Advisor Team
TECHNIQUES OF ANAESTHESIA FOR MAXILLARY General Considerations • Injections made on the buccal side of the tooth only anaesthetize the buccal mucosa. The Periodontal Ligament injection or local infiltration of the palatal gingiva is therefore required to anaesthetize the palatal gingiva for extractions. AFAMS Dental Advisor Team
TECHNIQUES OF ANAESTHESIA FOR MAXILLARY General Considerations • You must always be aware of the possibility of a hematoma when infiltrating posterior to the permanent molars due to the proximity of the venous plexus. (patient will feel burning) • 27 or 30-gauge short needle is normally used for all injections in the maxilla. AFAMS Dental Advisor Team
LOCAL INFILTRATION INJECTION IN THE MAXILLA • Technique • It may help to palpate the underlying bone before the needle is inserted because the root contour of the anterior teeth can usually be felt, and this ensures a more accurate injection. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK General Conditions • Mandible has very dense bone, except young children when it can be more porous. • Anaesthetic will therefore not diffuse through the cortical plate very readily. Therefore, a mandibular block is normally employed for all operative/surgical procedures. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK • The success of a mandibular block lies in the ability to palpate certain anatomical landmarks on the ramus. A thorough understanding of the surrounding anatomy is essential. • Note the position of the IAN in the adult versus the child Teeth Involved • All the teeth in one mandibular quadrant.
INFERIOR ALVEOLAR NERVE BLOCK Nerves Anaesthetized • Inferior Alveolar nerve and the Lingual Nerve. Indications • All operative and surgical procedures in the mandible. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Technique • 27-gauge long needle; two carpules are used for adult anaesthesia of the inferior alveolar nerve. • Bevel towards the bone, although for a block this is not critical. • The patient is in the supine position. The operator is seated on the chairside stool. • With the thumb or index finger of the left hand, palpate the internal and external oblique ridges on the anterior border of the ramus. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Pterygomandibularraphe Technique • Move the thumb or finger up and down on the ridges until the greatest depth of the anterior border of the ramus is identified. • With the thumb or finger still contacting the ridges and in the greatest depth of the notch, it is moved buccally to move the buccal sucking pad and give greater visibility. • The thumb or finger rests on the external oblique ridge. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Technique • The puncture point is made from the opposite side of the mouth with the syringe over the second premolar. • The puncture point is ¾ the distance from the external oblique ridge to the pterygomandibularraphe of the deepest point of the coronoid notch. • Small amounts of anaesthetic are deposited as the needle is slowly advanced until it contacts the bone of the ramus. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Technique • At this point normally only ½ to ¾of the length of the needle should be buried in the tissue when it contacts the bone. • If more than ¾ is buried, the injection is likely too deep. • If less than ½ of the needle is buried, the injection is too shallow. In both cases anaesthesia will be inadequate. ¾ of needle is buried AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Technique • The needle is backed off ½ millimeter and the syringe is aspirated to make sure the inferior alveolar artery or vein has not been punctured. • ¾ of a carpule of anaesthetic is then deposited. • The needle is withdrawn to half the buried depth. Aspirate and deposit the remaining ¼ carpule to anaesthetize the lingual nerve. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Technique • With a new carpule, landmark and deposit another ¾ carpule for the inferior alveolar nerve and without removing the syringe from the mouth, withdraw the needle and hop over the occlusion, and deposit the remaining ¼ carpule to anaesthetize the long buccal nerve. • It is common practice to use two carpules for adults in performing the inferior alveolar nerve block. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Symptoms of Anaesthesia • Lower lip and chin feel fat, thick, or rubbery on the side of the injection. • Complete numbness of the lateral side of the anterior ⅔ of the tongue on the side of the injection. • If the symptoms are not present or are only slight, then the block is not profound enough for operative or surgical work and the technique should be re-evaluated before re-injecting to see if your initial landmarks were incorrect. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Reasons for Failure • Poor technique – strict adherence to the anatomical landmarks is vital for success of the injection. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Reasons for Failure • Injecting too high – if the needle of the syringe is directed too high, there is a possibility of puncturing one of the blood vessels leading down to the mandibular canal. This may result in a hematoma. There is also the possibility of anaesthetizing the auriculotemporal branch of the mandibular division that supplies the temporal region of the head. Injecting too high carries a higher risk of success than injecting too low. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Reasons for Failure • Injecting too low – if the needle of the syringe is directed too low, usually complete failure of the block results without any of the classic signs of anaesthesia because the solution has been deposited below the lingula. The sphenomandibular ligament prevents diffusion of the local anaesthetic to successfully anaesthetize the inferior alveolar nerve. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Reasons for Failure • Injecting too deep – if more than ¾ of the needle disappears into the tissue before the bone is palpated, it means that the needle is too deep and has probably entered into the parotid gland which could possibly result in anaesthesia of the facial nerve with subsequent drooping of the eyelid, asymmetric smile, etc., due to temporary paralysis of the muscles of facial expression. AFAMS Dental Advisor Team
INFERIOR ALVEOLAR NERVE BLOCK Reasons for Failure • If pain is felt during injection it means: • You are injecting a volume of anaesthetic too quickly. • You have pushed the needle through the medial pterygoid muscle instead of into the pterygomandibular triangle. • The tip of the needle is sliding along the bone and tearing the periosteum. • The needle has contacted either the lingual or inferior alveolar nerve. This results in an “electric shock” like sensation. AFAMS Dental Advisor Team
Long Buccal Nerve Injection Nerve Anaesthetized : • Long Buccal Nerve Indication • This injection is in addition to the mandibular nerve block and is usually routinely given in order to anaesthetize the buccalgingiva in the molar region. The nerve itself runs from the distobuccal side of the third molar to the mesio-buccal side of the first molar. It is done for all operative and surgical procedures in the area. AFAMS Dental Advisor Team
Long Buccal Nerve Injection Technique • Since this injection is in addition to the mandibular nerve block, there is already a long 27-gauge needle in the syringe. A quarter of a carpule of anaesthetic is usually sufficient. • With the bevel facing down, puncture the muco-buccal fold at a point just posterior and lateral to the third molar tooth at the level of the C-E junction. • Deposit ¼ carpule of anaesthetic with the needle held parallel to the body of the mandible. AFAMS Dental Advisor Team
Long Buccal Nerve Injection Symptoms of Anaesthesia • Test the area with the sharp end of an explorer, as no painful sensation will be felt with successful anaesthesia. AFAMS Dental Advisor Team
Long Buccal Nerve Injection AFAMS Dental Advisor Team
Periodontal Ligament Injection • Position the patient • A 27 gauge needle is preferred • Apply topical for at least 1 minute unless the area is already numb • Stabilize the syringe • Orient the needle along the long axis of the tooth • Place the bevel against the tooth first on the mesial side (then repeat this on the distal) and insert into the periodontal sulcus until resistance is met
Periodontal Ligament Injection • Slowly deposit approximately 0.2 ml of local anaesthetic • You will feel resistance as you inject • You should notice blanching of the tissue
Children's Teeth • The same injections and techniques apply to the deciduous dentition as to the permanent one. • The only variation is that canine, as well as the central and lateral teeth in the mandible can be anaesthetized with a local infiltration technique, but it is usually preferable to anaesthetize the first and second deciduous molars with a mandibular block. • Mlp stuff AFAMS Dental Advisor Team
سوالات؟ Questions? UNCLASSIFIED//REL TO NATO/ISAF