Download
1 / 21
230 likes | 369 Vues
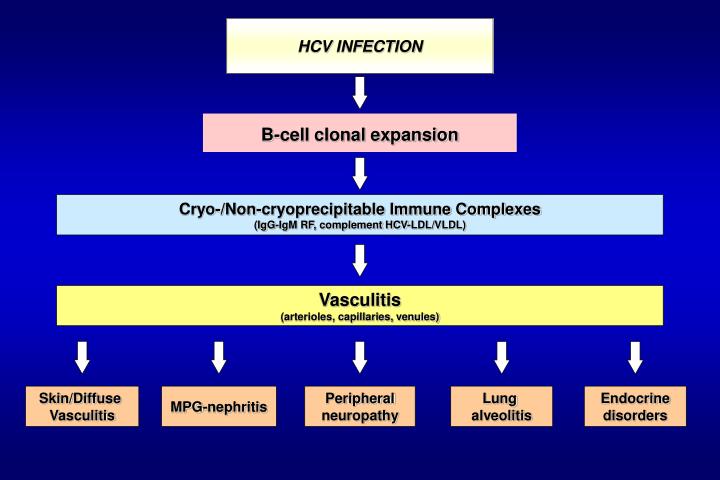
HCV INFECTION. B-cell clonal expansion. Cryo-/Non-cryoprecipitable Immune Complexes (IgG-IgM RF, complement HCV-LDL/VLDL). Vasculitis (arterioles, capillaries, venules). Skin/Diffuse Vasculitis. MPG-nephritis. Peripheral neuropathy. Lung alveolitis. Endocrine disorders.

E N D
HCV INFECTION B-cell clonal expansion Cryo-/Non-cryoprecipitable Immune Complexes (IgG-IgM RF, complement HCV-LDL/VLDL) Vasculitis (arterioles, capillaries, venules) Skin/Diffuse Vasculitis MPG-nephritis Peripheral neuropathy Lung alveolitis Endocrine disorders
MC Therapeutic Strategies * selective B-cell suppression
IFN MONOTHERAPY IN HCV-RELATED MC AUTHOR n° patients TREATMENT (IFN MIU) RESPONSE ETR 87% SR 0% ETR100% SR 0% ETR 50% ETR 75% ETR 60% SR 0% ETR 53% SR 25% IFN; 33% IFN+CS ETR 0% ETR 28% ETR 28 or 39% SR 11 or 22% ETR 52% ETR 60% SR 9% ETR 65% SR 33% ETR 62% Ferri, 1993 Ferri, 1993 Marcellin, 1993 Johnson, 1993 Misiani, 1994 Dammacco et al,1994 Johnson, 1994 Mazzaro, 1994 Mazzaro,1995 Casaril, 1996 Cohen, 1996 Akriviadis, 1997 Casato, 1997 15 26 2 4 MPGN 27 31: 16 with CS 14 MPGN 18 36 25 20 20 31 2/d(1m)- 2x3/w (5m) 2/d(1m)- 2x2/w (5m) 3x3/w (6 m) 1-10 (2-12m) 1.5x3(1w)-3x3/w(23w) 3x3/w (12m) variable 3x3/w 3x3/w(6 or 12m) 6x3/w (6 m) 3x3/w 3-5x3/w(6-12 m) 3/d(3m)-3x3/w(>9m)
Ferri et al. Interferon- in Mixed Cryoglobulinemia Patients: a Randomized, Crossover-Controlled Trial. Blood 1993 Patients:26 MC (15 w/11m; mean age: 54 years); 22/26 received CS Study design: With IFN- Without IFN- Randomization 24-wk 24-wk 26 HCV MC Without IFN- With IFN- Therapy:IFN- 2x106 MIU/d for 1 mo 2x106MIUx3/w for 5 months Pre-treatment CS were maintained in 22 patients
Ferri et al. Interferon- in Mixed Cryoglobulinemia Patients: a Randomized, Crossover-Controlled Trial. Blood 1993 RESULTS Improvement of both clinical and serologic parameters in IFN treated pts vs no variation in clinical and serologic parameters in untreated pts -6/26 (23%) dropped out after 1-10 w. of IFN therapy - rapid MC relapse after IFN therapy: no MC SR - 2/15 virologic ETR, no SVR
MISIANI et al. IFN-2a therapy in cryoglobulinemia associated with HCV. NEJM 1994 Patients:53 HCV MC patients (about ¾ with renal involvement) Treatment:IFN 1.5 MIUx3/w for 1mo – 3 MIUx3/w for 5mo previous treatments were continued (CS in 26% group A and 27% group B pts) Study design: A-Treatment group: 27 pts. Randomization 60% 0% 24-48 mo f-u 24-wk 53 HCV MC 0% 0% B-Control group: 26 pts. Results:MC ETRMC SR
MISIANI et al. IFN-2a therapy in cryoglobulinemia associated with HCV. NEJM 1994 Clinical--biochemical and virological changes induced by IFN therapy were closely related: improvement of MC syndrome in pts with virologic ETR vs progressive deterioration of MC syndrome in most NR and control pts Changes in cryoprecipitate in treated pts according to virologic ETR All ETR pts experienced recurrence of serum HCV RNA positivity and worsening of MC
COMBINED IFN (recombinant or pegylated) + RBVIN HCV-RELATED MC AUTHOR Patients n° TREATMENT RESPONSE 3 MIU IFN x 3/w (12m) 3 MIU IFN x 3/w + RBV (12 m) 3 MIU IFN x 3/w + RBV (6 m) variable IFN + RBV (6-56 m) 3 MIU IFN x 3/w + RBV (12 m) 3 MIU IFN x 3 /w or Peg-IFN + RBV (> 18 m) 1.5 ug/Kg/w Peg-IFN + RBV (> 10 m) 1 ug/Kg/w Peg-IFN+ RBV (12 m) Calleja, 1999 Zuckerman, 2000 Cacoub, 2002 Mazzaro, 2003 Alric, 2004 Cacoub, 2005 Mazzaro, 2005 18 8 NR 9 NR 14 27 NR or relapsers 18 9 18 ETR 55% SR 28% ETR 63% SR 38% ETR 78% SR 22% SR 71% ETR 85% SR 70% SR 88% ETR 89% SR 44%
Zuckerman et al. J Rheumatol 2000 Patients: 9 MC patients who failed to respond to IFN monotherapy (8 NR and 1 Rel) HCV genotype: 1b or 1b+2a in 7/9 Treatment: IFN 3x3 MIU/w + RBV 1000-1200 mg/d for 6 months ( in 2 pts 1-3 months CS) Follow-up: 6-9 months Results: ET MC response: substantial improvement in all pts Follow-up: complete and sustained remission only in pts (2/9) with virologic response x: ALT : Cryocrit
Mazzaro et al. J Hepathol 2005 Patients:18 naïve MC patients: 15 type II - 3 type III; 11/18 HCV genotype 1 or 4 Treatment:Peg-IFN 1 μg/Kg/w + RBV 1000 mg/day for 6 months Follow-up:6 months Cacoub et al, Arthritis Rheum 2005 Patients:9 MC patients (7/9 naïve); 7 type II - 2 type III; 7/9 HCV genotype 1 Treatment:Peg-IFN 1.5 μg/Kg/w + RBV 800-1200 mg/day for at least 10 mo (10-26 mo) Follow-up:6 months Sustained MC Response (%) IFN 1μg/Kg + Riba IFN 1.5μg/Kg + Riba
MC EtiologicTherapy: IFN RBV • PROS • Antiviral + antiproliferative +immunomodulating effects • Useful in most studies • MC response was correlated with virologic response • Increased response was correlated with increased antiviral efficacy of treatment • Sustained clinical remission was only observed in patients with sustained virologic response • Pathogenetic value: • association between effects on • viral replication and clonal B-cell expansion • CONS • Difficult comparison between available studies (variability of protocols) • High frequency of relapse • Frequent contraindications • Difficult assessment of response: frequent discordance between serological MC and clinical MC as well as virologic parameters
Regression of B-cell clonal expansion after antiviral therapy Mazzaro et al.Regression of monoclonal B-cell expansion in patients affected by mixed cryoglobulinemia responsive to alpha-interferon therapy. Cancer 1996 In 3 out of 4 MC SR patients: disappearance of expanded B-cell clones -detected through IgH VDJ analysis of PBMC- as well as bone marrow monoclonal infiltrate Casato et al.Regression of lymphoproliferative disorder after treatment for HCV infection in a patient with partial trisomy 3, Bcl-2 overexpression, and type II cryoglobulinemia. Blood 2001 Effect of IFN therapy on viral titers and the prevalence of IgMk B cells
Regression of B-cell clonal expansion after antiviral therapy Association between B-cell t(14;18) and HCV MC Jh C Chr 14 B cell bcl-2 Chr 18 t(14;18) bcl-2 C Regression of t(14;18)+ B-cell clones after antiviral therapy Zuckerman et al. Blood 2001;97: 1555 Zignego et al. Ann Intern Med 2002; 137:571 Giannelli et al. Blood 2003;102:1196
Regression of B-cell clonal expansion after antiviral therapy Effect of antiviral therapy on determination of t(14;18)+ B-cell clones: MC and virologic ETR followed by relapse during post-treatment f-u Giannelli et al, Blood, 2003
Patients.79 HCV SVR : (A) 68 HCV+ CLD (B) 11 MC (9 IgG+IgMk; 2 IgG+IgMk+λ) • Mean f-u after therapy61 (15-107) months= • persistence of “occult” lymphatic infection in MC vs CLD: p<0.001 • t(14;18) in persistent lymphatic infection vs cleared HCV: p<0.001 Correlation between “occult” HCV lymphatic infection after antiviral therapy and MC persistence HCV + HCV + HCV + IFN + RBV NR SVR HCV - HCV - HCV + HCV - HCV - HCV - no MC persistence of MC Giannini et al. 41st EASL Annual Meeting, Vienna 2006
Saadoun et al.Splenic lymphoma with villous lymphocytes, associated with type II cryoglobulinemia and HCV infection: a new entity? Blood 2005 Patients: 18 SLVL HCV+; in 18/18 type II MC (13/18 MCS); HCV genotype 1 or 4 in 8/18 Treatment: IFN 3 MIUx3/w + Riba 1000-1200 mg/day for 6 mo in partial responders therapy prosecution until complete response: range of therapy duration 6-39 m Follow-up: mean 62 months 100% 100% 78% 22% *Hematologic and virologic response
HCV ? BL infection HCV mutagenesis HCV E2 - CD81 binding chronic infection HCV variability ? ? IFN + Riba t(14;18)/others? Bcl-2 overexpression B-cell apoptosis inhibition Polyclonal BL expansion + Genetic and/ or environmental factors (peculiar RF B cell stimulation) Prolonged B-cell survival MC Additional genetic aberrations Malignant NHL
Algorithm for treatment of HCV(+)-MC patients with antiviral therapy Evaluation of MC syndrome and ALT levels Asymptomatic MC Normal ALT Severe MC (i.e. acute nephritis, widespread vasculitis) NO antiviral therapy Symptomatic MC Asymptomatic MC Elevated ALT Normal ALT Elevated ALT Antiviral Therapy
MC Therapeutic Strategies * selective B-cell suppression
80 60 45 25 10 Anti-CD20 monoclonal antibody (rituximab) for the treatment of MC Rituximab is a human/mouse chimeric Mab that reacts with CD20 antigen present during different steps of the maturation of B lymphocytes Lamprechtet al, 2003 Roccatello et al, 2004 Ghijsels et al, 2004 Cervetti et al, 2005 Quartuccio et al, 2006 Petrarca et al, submitted Zaja F et al. 2002 Sansonno et al. 2003 Zaja et al, 2003 90 RITUXIMAB 80 • High frequency of MCS response 70 RESPONSE (%) 60 50 • Efficacy on BL clonal expansion 40 30 • Enhanced HCV viraemia/ALT titres 20 10 1 2 3 4 5 6 7 8 9 10 11 12 WEEKS MONTHS Suggested association with effective anti-viral agents PROBABILITY OF COMPLETE RESPONSE AFTER RITUXIMAB THERAPY Sansonno et al. Blood. 2003
Algorithm for management of MC(+) patients who resulted non-responders or in whom antiviral treatment was contraindicated or not tolerated Evaluation of MC syndrome severity Moderate-severe MPGN, skin vasculitis or Severe-rapidly progressive MPGN Severe sensomotor neuropathies Widespread vasculitis Mild-moderate purpura Weakness Arthralgias Mild neuropathy Rituximab PE + CS +/- CF LAC diet Low-medium doses CS +/- other symptomatics NON RESPONDERS RESPONDERS SEVERE MODERATE Antiviral therapy ?