Download
1 / 36
370 likes | 392 Vues
The PleurX peritoneal catheter drainage system for vacuum-assisted drainage of treatment-resistant, recurrent malignant ascites. Implementing NICE guidance. March 2012. NICE medical technology guidance 9. What this presentation covers. Background and definitions Guidance Discussion

E N D
The PleurX peritoneal catheter drainage system for vacuum-assisted drainage of treatment-resistant, recurrent malignant ascites Implementing NICE guidance March 2012 NICE medical technology guidance 9
What this presentation covers • Background and definitions • Guidance • Discussion • Accessing the guidance and implementation tools • Case studies
Background: medical technologies guidance • NICE medical technology guidance addresses specific technologies notified to NICE by manufacturers. • If the case for adopting the technology is supported, then the technology has been found to offer advantages to patients and the NHS. • The specific recommendations on individual technologies are not intended to limit use of other relevant technologies that may offer similar advantages.
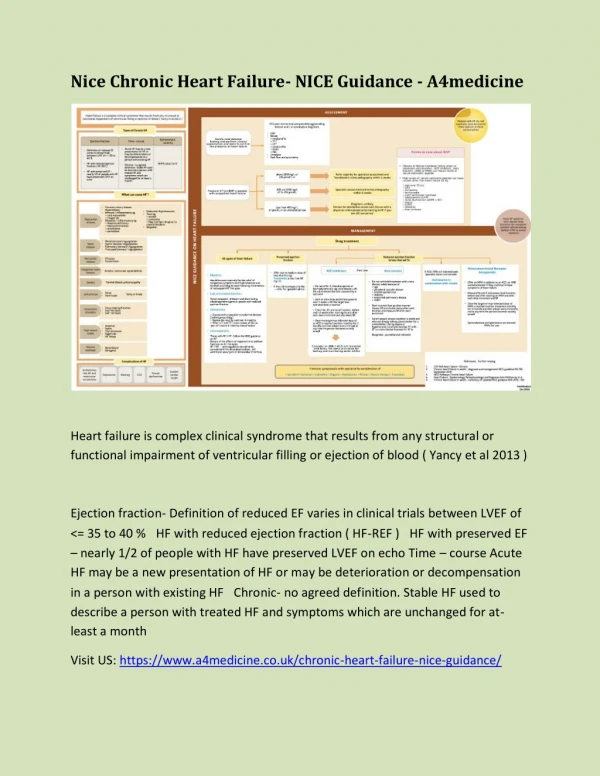
Definitions • Malignant ascites – an abnormal accumulation of fluid in the peritoneal cavity, caused by cancer. Symptoms include breathlessness, nausea, bloating, acid reflux, abdominal pain, reduced appetite, reduced mobility and psychological distress related to negative perception of body image • Treatment-resistant – there is a low likelihood of further medical or oncological interventions, in particular chemotherapy, being successful in preventing or reducing re-accumulation of ascites
Background: current clinical practice • Conventional management involves repeated large-volume paracentesis (inserting a catheter into the pertioneal cavity to drain ascitic fluid) • Most commonly done as an inpatient procedure. Some centres offer it as a day case procedure • In large volume paracentesis the catheter stays in placeuntil most of the ascites has drained. Some patients may need to stay in hospital for one or more nights for repeated drainage procedures.
Background: The PleurX peritoneal catheter drainage system for vacuum-assisted drainage • Allows palliative management of treatment-resistant, recurrent malignant ascites in the community setting • Comprises a silicone catheter and a drainage system containing a vacuum bottle and drainage line • The catheter can remain in place indefinitely • Patients and carers are trained to perform drainage • To drain, the vacuum bottle is attached to the catheter. A fresh valve cap and dressing are applied once the drainage is completed
Guidance (1) • The case for adopting the PleurX peritoneal catheter drainage system in the NHS is supported by the evidence. • Evidence and cost modelling suggests that the PleurX peritoneal catheter drainage system: • is clinically effective • has a low complication rate • has the potential to improve quality of life • enables early treatment of symptoms in the community • is cost saving compared with inpatient large-volume paracentesis Reproduced with permission from UK Medical Ltd
Guidance (2) The PleurX peritoneal catheter drainage system should be considered for use in patients with treatment-resistant, recurrent malignant ascites Reproduced with permission from CareFusion Corporation
Management in the community • The device is not likely to increase the need for community nursing support because most patients in the terminal stages of cancer will receive healthcare in the community • The need for community nursing may be reduced slightly, as the nursing wound management associated with large volume paracentesis will not be needed • Training is required for community nurses, patients and carers to perform community drainage
Discussion • How can we prepare a case for the organisation to invest in this technology? • Where can we access further training resources to support the implementation of this guidance in practice? • Where a healthcare professional identifies a patient that may benefit from this device do we have systems in place for referral and further consideration of suitability? If not, how can we develop these? • How can we encourage local commissioners to support the use of this device?
Accessing the guidance and implementation tools online • Visit www.nice.org.uk/guidance/MTG9 for • Guidance • Costing tools • Audit support • Podcast • Clinical case scenarios (PDF) Reproduced with permission from UK Medical Ltd
Case studies • The decision to start treatment with the PleurX peritoneal catheter drainage system should be shared between clinicians and patients • These case studies have been have been put together to improve your ability to identify people who would potentially benefit from using the PleurX peritoneal catheter drainage system for vacuum-assisted drainage. They are aimed at oncologists and oncology clinical nurse specialists but could be used to support learning in a variety of healthcare professionals responsible for caring for people with cancer. • These cases are also available in PDF format for individual learning Disclaimer: these case studies, their content and suggested actions are not NICE guidance. They have been developed in collaboration with experts in the field to support learning but they are beyond the scope of the guidance
Case scenario 1: Stephen • Presentation • Stephen is a 68-year-old man with advanced colon cancer. You are Stephen’s community palliative nurse specialist. Stephen is complaining of bloating, nausea, acid reflux and reduced appetite which you believe to be caused by ascites. He underwent large volume paracentesis 20 days ago, and 5 litres of ascites were drained. Prior to this he has never had paracentesis. Stephen's oncologist considers him to have 'treatment-resistant' cancer with malignant ascites. • Question 1.1 • Should the PleurX peritoneal catheter drainage system • be considered for Stephen?
Case scenario 1: Stephen • Answer 1.1 • Yes, the PleurX peritoneal catheter should be considered for Stephen as his cancer is considered to be 'treatment-resistant' with 'malignant ascites' and it is possible that his ascites has re-accumulated. However, the Committee recognised the uncertainty about the point in the care pathway at which it would be clinically appropriate to treat patients with treatment-resistant, recurrent malignant ascites with the PleurX peritoneal catheter drainage system. Tapping et al. (2011) considered that patients who had at least three previous large-volume paracentesis procedures would be suitable for treatment with the PleurX peritoneal catheter drainage system, whereas Courtney et al. (2008) inserted the PleurX peritoneal catheter in patients who had had at least two large-volume paracentesis procedures in the previous 30 days. • The Committee did not recommend a minimum number of re-occurrences of ascites before it would be clinically appropriate to treat with the PleurX peritoneal catheter drainage system. They considered that the decision to start treatment with the PleurX peritoneal catheter drainage system should be shared between clinicians and patients.
Case scenario 1: Stephen • Question 1.2 • What are the options for Stephen?
Case scenario 1: Stephen • Answer 1.2 • There are two options here. Stephen could undergo repeat large volume paracentesis with further monitoring of symptoms and re-accumulation of ascites, leaving open the option for treatment with the PleurX peritoneal catheter drainage system when this happens. Alternatively, if Stephen's multidisciplinary team believes it is clinically appropriate to use the PleurX peritoneal catheter drainage system at this stage and Stephen is in agreement, Stephen could begin treatment with the PleurX peritoneal catheter drainage system immediately. • As Stephen’s community palliative care nurse it is important that you discuss these options with Stephen and the relevant members of his multidisciplinary team. • Questions 1.3 • If a decision is made between Stephen and his multidisciplinary team to use the PleurX peritoneal catheter drainage system how could you help with this process?
Case scenario 1: Stephen • Answer 1.3 • It could be suggested that prior to insertion of the device the appropriate healthcare professionals in Stephen's multidisciplinary team should contact the relevant GP and community healthcare team to ensure they have the skills and resources to support Stephen. • The NICE costing tools can help you to calculate the anticipated local costs and savings associated with implementing this guidance. • The manufacturer provides training and learning resources to support use of this device including patient leaflets, instruction booklets and videos. These resources are available from www.ukmedical.com/pleurx. Note that this webpage also provides details of other uses of ‘PleurX devices’. This guidance only covers the use of the PleurX peritoneal catheter drainage system for vacuum-assisted drainage of treatment-resistant, recurrent malignant ascites.
Case scenario 2: Julie • Presentation • Julie is a 58-year-old woman who has been diagnosed with stage 4 ovarian cancer and has been offered primary chemotherapy. She has been found to have moderate volume ascites as well as pleural effusion on a CT (computed tomography) scan but is currently asymptomatic. She will commence carboplatin and paclitaxel chemotherapy next week • Question 2.1 • Should the PleurX peritoneal catheter drainage system be considered for Julie?
Case scenario 2: Julie • Answer 2.1 • No, because although ascites has been found on Julie's CT scan she is asymptomatic. The purpose of the PleurX peritoneal catheter drainage system is symptom relief. If she does not need symptom relief then treatment with the PleurX peritoneal catheter drainage system is not suitable for her. Additionally, she is scheduled to start chemotherapy, which is expected to prevent further accumulation of ascites. Her condition is therefore not yet considered to be 'treatment-resistant‘*. Although her ascites is likely to be malignant the PleurX peritoneal catheter drainage system would not be considered suitable for her at this stage. • * see notes
Case scenario 3: Suzanne • Presentation • Suzanne is a 68-year-old woman who is attending an oncology clinic after discovery of a pelvic mass and ascites by her gynaecology team. Tissue biopsy has confirmed incurable metastatic lobular breast carcinoma. She has been offered endocrine therapy. She has marked shortness of breath and nausea which are considered to be associated with the ascites. Her ascites was drained 10 days ago and clinically has now recurred. • Question 3.1 • Should the PleurX peritoneal catheter drainage system be considered for Suzanne?
Case scenario 3: Suzanne • Answer 3.1 • Suzanne has been offered treatment with endocrine therapy. It is anticipated that the endocrine therapy may relieve the ascites. Therefore, although Suzanne's ascites could be considered malignant her condition is not yet considered ’treatment-resistant’. The PleurX peritoneal catheter drainage system is therefore not considered suitable for her at this stage. For symptom relief large-volume paracentesis should be suggested. • If the endocrine therapy does not treat the ascites then the PleurX peritoneal catheter drainage system should be considered.
Case scenario 4: John • Presentation • John is a 54-year-old man with pancreatic cancer. The multidisciplinary team considers that his cancer is incurable and is not suitable for surgical resection or radical radiotherapy. Palliative chemotherapy did not prevent disease progression. His notes indicate that there is a low likelihood of further medical or oncological interventions, in particular chemotherapy, being successful in preventing or reducing re-accumulation of ascites. You are the oncology nurse specialist working in the oncology ward where John has been admitted as an unplanned inpatient for large volume paracentesis. During the ward round you note that this is John’s third admission for large volume paracentesis in 35 days. The need for repeated paracentesis is the main barrier to John receiving care at home. • Question 4.1 • Should the PleurX peritoneal catheter drainage system be considered for John?
Case scenario 4: John • Answer 4.1 • Yes, the PleurX peritoneal catheter should be considered for John. NICE recommends that the PleurX peritoneal catheter drainage system should be considered for use in patients with treatment-resistant, recurrent malignant ascites. The Committee concluded from the available clinical evidence that the PleurX peritoneal catheter drainage system is effective in the palliative management of treatment-resistant, recurrent malignant ascites. It has a high procedural success rate, a low complication rate and the potential to improve patient quality of life • There is no definition in the guidance as to what ‘recurrent’ is and the Committee recognised the uncertainty about the point in the care pathway at which it would be clinically appropriate to treat suitable patients with the PleurX peritoneal catheter drainage system. Tapping et al. (2011) considered that patients who had at least three previous large-volume paracentesis procedures would be suitable for treatment with the PleurX peritoneal catheter drainage system, whereas Courtney et al. (2008) inserted the PleurX peritoneal catheter in patients who had had at least two large-volume paracentesis procedures in the previous 30 days. Answer continued on next slide
Case scenario 4: John • Answer 4.1 continued • The Committee did not recommend a minimum number of re-occurrences of ascites before it would be clinically appropriate to treat with the PleurX peritoneal catheter drainage system. They considered that the decision to start treatment with the PleurX peritoneal catheter drainage system should be shared between clinicians and patients. In light of this information you and the multidisciplinary team should consider the PleurX peritoneal catheter drainage system for John. • Question 4.2 • What would you do next?
Case scenario 4: John • Answer 4.2 • You should first discuss this treatment option with the relevant members of John's multidisciplinary team. • When developing the guidance the Committee considered that the decision to start treatment with the PleurX peritoneal catheter drainage system should be shared between clinicians and patients. You should discuss this option with John and his carers so that he and the multidisciplinary team can make a joint decision. • It could also be suggested that prior to insertion of the device the appropriate healthcare professionals in John’s multidisciplinary team should contact the relevant GP and community healthcare team to ensure they have the skills and resources to support John. • Answer continued on next slide
Case scenario 4: John • Answer 4.2 continued • The NICE costing tools can help you to calculate the anticipated local costs and savings associated with implementing this guidance. • The manufacturer provides training and learning resources to support the use of the device including patient leaflets, instruction booklets and videos. These resources are available from www.ukmedical.com/pleurx. Note that this webpage also provides details of other uses of ‘PleurX devices’. This guidance only covers the use of the PleurX peritoneal catheter drainage system for vacuum-assisted drainage of treatment-resistant, recurrent malignant ascites.
Case scenario 5: Doris • Presentation • Doris is a 75-year-old woman. You are her oncologist. She was diagnosed with stage IV ovarian cancer 3 years ago. She has had surgery and multiple types of chemotherapy. Doris is attending your clinic today and you need to report on her latest CA125 levels. The result indicates her cancer has progressed again. There are no further treatment options available to Doris which would reduce the ascites. She has been admitted for inpatient large volume paracentesis twice in the past 25 days, and on each occasion 5–6 litres of ascites were drained. • On presentation Doris is complaining of shortness of breath and nausea. • Question 5.1 • If these symptoms were confirmed as ascites would you consider the PleurX peritoneal catheter drainage system for Doris?
Case scenario 5: Doris • Answer 5.1 • Yes, the PleurX peritoneal catheter drainage system should be considered for Doris. NICE recommends that the PleurX peritoneal catheter drainage system should be considered for use in patients with treatment-resistant, recurrent malignant ascites. However, the Committee recognised the uncertainty about the point in the care pathway at which it would be clinically appropriate to treat patients with treatment-resistant, recurrent malignant ascites with the PleurX peritoneal catheter drainage system. Tapping et al. (2011) considered that patients who had at least three previous large-volume paracentesis procedures would be suitable for treatment with the PleurX peritoneal catheter drainage system, whereas Courtney et al. (2008) inserted the PleurX peritoneal catheter in patients who had had at least two large-volume paracentesis procedures in the previous 30 days. • Answer continued on next slide
Case scenario 5: Doris • Answer 5.1 continued • In current practice some clinicians would not offer it as a treatment option until the ascites has re-occurred three times. However, the Committee did not recommend a minimum number of re-occurrences of ascites before it would be clinically appropriate to treat with the PleurX peritoneal catheter drainage system. They considered that the decision to start treatment with the PleurX peritoneal catheter drainage system should be shared between clinicians and patients. In light of this information you and the multidisciplinary team should consider the PleurX peritoneal catheter drainage system for Doris. • Question 5.2 • What would you do next?
Case scenario 5: Doris • Answer 5.2 • The most appropriate course of action depends on how short of breath she is. If the ascites is leading to significant respiratory compromise then it may be appropriate to admit her to hospital acutely and perform urgent paracentesis to relieve her shortness of breath. • If her shortness of breath is not severe then sufficient time should be taken to discuss both the PleurX peritoneal catheter drainage system and repeated large-volume paracentesis and allow Doris to make an informed choice between the two. A joint decision on treatment should be made by Doris and her multidisciplinary team. • If the decision is made to use the PleurX peritoneal catheter drainage system it could be suggested that prior to insertion of the device, the appropriate healthcare professionals in Doris's multidisciplinary team should contact the relevant GP and community healthcare team to ensure they have the skills and resources to support Doris. • Answer continued on next slide
Case scenario 5: Doris • Answer 5.2 continued • The NICE costing tools can help you to calculate the anticipated local costs and savings associated with implementing this guidance. • The manufacturer provides training and learning resources to support the use of the device including patient leaflets, instruction booklets and videos. These resources are available from www.ukmedical.com/pleurx. Note that this webpage also provides details of other uses of ‘PleurX devices’. This guidance only covers the use of the PleurX peritoneal catheter drainage system for vacuum-assisted drainage of treatment-resistant, recurrent malignant ascites.
Case scenario 6: Jane • Presentation • Jane is a 58-year-old woman diagnosed with stage III ovarian cancer. She is experiencing bloating, acid reflux and reduced appetite, which is thought to be caused by ascitic fluid. You are a gynaecology oncology clinical nurse specialist and Jane is attending your preoperative clinic. She is booked for surgery in two weeks’ time with the objective of surgical staging and complete resection of all macroscopic disease, followed by chemotherapy. • Question 6.1 • Should the PleurX peritoneal catheter drainage system be considered for Jane?
Case scenario 6: Jane • Answer 6.1 • No, the symptoms listed above are not necessarily caused by large volume ascites – there could be peritoneal disease or bowel involvement. • If it were to be established that these symptoms were caused by ascites the PleurX peritoneal catheter drainage system should still not be considered at this stage because it is recommended by NICE for consideration in people with treatment-resistant, recurrent malignant ascites. Jane's condition is not yet considered 'treatment-resistant’ as it is anticipated that the planned surgery and chemotherapy will treat the ascites and prevent further accumulation. • In this case if Jane had had a tense abdomen with confirmed ascites she would have received paracentesis in advance of surgery.
Clinical case scenarios references and acknowledgements • References • Becker G, Galandi D, Blum H E (2006) Malignant ascites: systematic review and guideline for treatment. European Journal of Cancer 42 (5) 589–97 • Courtney A, Nemcek A AJr, Rosenberg S et al. (2008) Prospective evaluation of the PleurX catheter when used to treat recurrent ascites associated with malignancy. Journal of Vascular & Interventional Radiology 19 (12) 172331 • Tapping C R, Ling L, Razack A (2011) PleurX drain use in the management of malignant ascites: safety, complications, long-term patency and factors predictive of success. British Journal of Radiology 2011 Mar 22. [Epub ahead of print] • Acknowledgements • NICE would like to thank the members of the Medical Technologies Advisory Committee, in particular Dr Alex Faulkner. • We would also like to thank the following people: • Dr. Hans-Ulrich Laasch, Consultant Radiologist & Interventional Lead, The Christie NHS Foundation Trust • Alison Keen, Interim Head of Cancer Nursing, University Hospital Southampton NHS Foundation Trust • Dr Peter Hall, Specialist Registrar/Clinical Research Fellow, Leeds Teaching Hospitals NHS Trust/University of Leeds
What do you think? • Did the implementation tool you accessed today meet your requirements, and will it help you to put the NICE guidance into practice? • We value your opinion and are looking for ways to improve our tools. Please complete this short evaluation form. • If you are experiencing problems accessing or using this tool, please email implementation@nice.org.uk To open the links in this slide set right click over the link and choose ‘open link’
Clinical case scenarios definitions • Malignant ascites is defined as abnormal accumulation of fluid in the peritoneal cavity, caused by cancer. It is most commonly associated with breast, lung, ovary, stomach, pancreas and colon cancer (Becker et al. 2006). The accumulation of a large volume of ascitic fluid increases abdominal pressure and can cause symptoms such as breathlessness, nausea, bloating, acid reflux, reduced appetite, reduced mobility and psychological distress related to negative perception of body image (Becker et al. 2006). Patients with malignant ascites have a mean survival of 1–4 months, depending on the nature and extent of the underlying tumour (Courtney et al. 2008). Patients having palliative treatment may survive significantly longer. • Treatment-resistant : The Committee was advised that the term ‘treatment-resistant’ is normally understood by clinicians to mean that there is a low likelihood of further medical or oncological interventions, in particular chemotherapy, being successful in preventing or reducing re-accumulation of ascites Return to case 1 - presentation Return to answer 1.1 Return to answer 2.1 Return to answer 3.1 Return to answer 6.1