Download
1 / 94
940 likes | 981 Vues
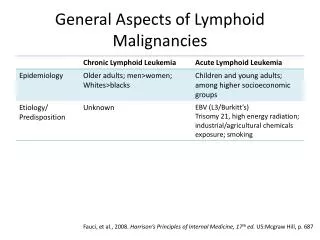
Low grade B cell Lymphoid Malignancies (LGBLM). This term is used to describe mainly 2 major disease entities of adults and elderly (median age >50) that originate from mature (predominantly small) B lymphocyte. Indolent B cell NHL. B cell CLL. REAL/WHO Classification. Precursor B-Cell

E N D
Low grade B cell Lymphoid Malignancies (LGBLM) This term is used to describe mainly 2 major disease entities of adults and elderly (median age >50) that originate from mature (predominantly small) B lymphocyte Indolent B cell NHL B cell CLL
REAL/WHO Classification • Precursor B-Cell • B lymphoblastic • Mature (Peripheral) B-Cell • B-cell CLL/small lymphocytic lymphoma • Follicular lymphoma [Grades I, II , III] • Marginal zone B-cell lymphoma • MALT type • Nodal marginal zone B-cell lymphoma • Splenic marginal zone B-cell lymphoma • Lymphoplasmocytic lymphoma (immunocytoma) • Mantle-cell lymphoma • Diffuse large B-cell lymphoma • Burkitt lymphoma • Precursor T-Cell • T lymphoblastic • Mature (Peripheral) T-Cell • Mycosis fungoides/Sezary syndrome • Adult T-cell lymphoma/leukemia • Peripheral T-cell lymphoma, not otherwise specified • Angioimmunoblastic T-cell lymphoma • Anaplastic large T/null-cell lymphoma • Entranodal nasal NK/T-cell lymphoma • Enteropathy type T-cell lymphoma • Hepatosplenic gd T-cell lymphoma • Subcutaneous panniculitic-like T-cell lymphoma Adapted from Harris et al. Blood, 84: 1361, 1994 & Harris et al. JCO 17: 3835, 1999
Low Grade B Cell LymphomaFrequency and Diagnostic Accuracy Type Frequency Accuracy Follicular center cell 22% 94% Marginal zone B-cell, MALT 8% 86% Marginal zone B-cell, nodal 2% 63% Small lymphocytic/CLL 7% 87% Lymphoplasmocytoid 1% 56% 40% Adapted from Harris et al. Blood; 84: 1361, 1994
Low Grade B cell Lymphoma according to the last WHO classification 2008. Adapted from Harris et al 2008
Low Grade B cell Lymphoma Is it equally common throughout the world An EGYPTIAN large study (1009 cases) Frequency of Low Grade B cell Lymphoma : 8% Follicular subtypes : 5% Azim et al. Proc ASCO; abs#72, 1998
Low grade B cell Lymphoid Malignancies (LGBLM) Similarities • Natural History / Biological behavior • Treatmentresponse and outcome
LGBLM Natural History & Biology Histological transformation to high grade lymphoma observed in 30-40% of follicular lymphoma and 5-10% of SLL/CLL Spontaneous remission (20%) especially in low grade follicular lymphoma Tendency for Acker et al. JCO ;1:11, 1983 Horning and Rosenberg N Engl J Med ;311: 1471, 1984
LGBLMNatural History and Biology • BM and peripheral blood involvement is common because the mature B lymphocytes retain their normal ability to traffic throughout the lymphatic system and hence the majority of patients have an advanced stage at the time of diagnosis Grogan Ann Oncol7; (suppl 6): 3, 1996
LGBLM Natural History & Biology The vast majority of neoplastic B cells are non proliferating i.e In the Go phase (Quiescent phase) of the cell cycle e.g. 99% of B CLL cells are in the Go phase at the time of diagnosis Caligaris Cappio et al. JCO 17: 399, 1999
LGBLM Natural History & Biology Disease progression is mediate (at least initially) via gradual accumulation of malignant mature B lymphocytes rather than rapid proliferation. These cells enjoy a selective survival advantage relative to their normal counterparts e.g. CD5 +ve B cells has an average ½ life of 5-7 days versus several weeks-months in case of CLL/SLL Maclenna & Gray Immunol; Rev91: 61, 1986
LGBLMNatural History and Biology Cells Refusing to Die Majority of follicular NHL have genetic abnormality involving translocation between chromosomes 14 and 18 [t (14 ; 18) ( q 32 ; q 21)] Overexpression of BCL-2 gene (originally on chromosome 18) BCL-2 is an anti-apoptotic protein Korsmyer Blood; 80: 879, 1992
Translocation between chromosomes 14 and 18 [t (14 ; 18) ( q 32 ; q 21)] which results in BcL2 overexpression This brings the BCL2 gene under the control of immunoglobulin heavy chain gene (IgH) enhancers and leads to overexpression of BCL2 protein
LGBLM Cells refusing to die Cells Refusing to Die The t(14 ; 18) translocation (seen in the majority of follicular lymphoma) is exceedingly rare in SLL/CLL. However BCL-2 protein is consistently over expressed in these cells. Furthermore SLL/CLL do not respond to extra cellular apoptotic signals Caligamis Cappio et al. JCO 17: 399, 1999
LGBLM Treatment Response/Outcome The majority of LGBLM are quite sensitive to radiotherapy and wide range of chemotherapeutic drugs including: Alkylating agent, Corticosteroids, Anthracyclines & Purine analogs Induction of remission is high especially in chemo-naive patients. However CRs are not as highly seen in aggressive lymphoma. More frequent CRs are encountered in follicular lymphoma compared to other subtypes of LGBLM
LGBLM Treatment Response/Outcome The major therapeutic challenges in these disease is the maintenance of remission (not the induction of remission) as almost all the patients in remission would subsequently relapse ( + histologic transformation ) Because of eventual relapse no curative treatment has been established before the era of Rituximab.
Low grade B cell lymphomaManagement of advanced stage Treatment strategy • No prospective study has shown that treatment of asymptomatic patients (low tumor burden) at the time of diagnosis would prolong survival.
Treatment of indolent lymphoma NCI study 45 patients initial aggressive therapy (ProMace/Mopp) followed by total lymphoid irradiation VS 44 patients were observed, No initial therapy (Watch &Wait) Conclusion No survival advantage over Watch & Wait Young et al Semin. Hematol 25: 11, 1988 .
Indications to initiate treatment in LGBLMGELF criteria (High tumor Burden) Leukemia or blood cytopenia Mass > 7cm Nodal sites > 3 (3cm) Constitutional symptoms Substantial spleenomegaly Ureteric/mediastinal/epidural compression Serous effusion Solal Celigny P et al. N Engl Med;329: 1608, 1993
Follicular Lymphoma International Prognostic Index (FLIPI) The best predictive five parameters Age > 60 HB < 12 gm Stage III/IV Number of nodal sites 5 or more Increased LDH The records of 1795 patients with full clinical and 10 years survival data from Europe , North America and some far east countries were used to construct this prognostic model.
The Follicular Lymphoma International Prognostic Index (FLIPI): Overall survival 1.0 Good (01) 0.8 Intermediate (2) 0.6 Poor (35) Probability of survival 0.4 0.2 Months P < 0.0001 N = 1,795 0 0 12 24 36 48 60 72 84 Solal-Céligny P, et al. Blood 2004; 104:12581265.
For many decades, the standard therapy for symptomatic low grade B cell lymphoid malignancies (low grade lymphoma and CLL) was based on alkylating agents (usually chlorambucil)with or without prednisone The triple combination of cyclophosphamide, vincristine and prednisone (CVP) and /or external beam radiotherapy have been recommended if rapid response is required for relief of sever symptoms Treatment of LGBLM Symptomatic patients/high tumor burden Portlock CS Semin Oncol; 17(1):51, 1990
Treatment of LGBLM Anthracycline based regimens can produce higher response rates (and CRs) compared to CVPorChlorambucil. However no improvement in long-term disease free or overall survival has been demonstrated. Vose Ann Oncol 7; (suppl 6):13, 1996
Conventional Chemotherapies Overall survival of patients treated with cyclophosphamide vs. CHOP-Bléo (from Peterson et al.,JCO 2003)
The positive impact of adding alfa-Interferon to ADR based regimen in follicular lymphoma with high tumor burden (GELF-86 Trial) N=123 N=119 Solal-Celignc et al. JCO 16(7): 2332, 1998
Meta analysis of 10 randomized studies evaluating the role of interferon in follicular lymphoma 2005 cases at a median follow up period of 7 years Conclusions Addition of Interferon alpha did significantly improve survival incase of: Use of relatively intensified chemotherapy (ADR or Mitoxantrone based regimens) Adequate dose of interferon alpha ( ≥ 5 million unit per injection and ≥ 36 million unit / month) Rohatiner et al. Proc. ASCO; abs#1053, 2002
Purine AnalogsRational for use in LGBLM • They have unique Cytotoxicity against both dividing and non dividing lymphocytes (Go phase) Seto et al J Clin Inves. 75; 377, 1985 • They can initiate programmed cell death • Potential synergy with other useful drugs: cyclophosphamide & mitoxantrone Carson& Ribeiro Lancet 341; 1251, 1993 Koel et al. Proc AACR38 : 2; abs#10,1997
Fludarabine monotherapy in low grade lymphoma Previously Treated Response rate 40-50% CR 12-15% Redman et al. JCO 10:790, 1992 Hiddman e al. Semin Oncol 20; (suppl7): 28, 1993 Response rate 65-70% CR 35% Previously untreated Solal-Celigny et al. JCO14: 514, 1996 Pigaditou et al. Semin Oncol 20;(suppl 7): 24, 1993
Fludarabine is particularly effective in LGLwhile it has a much lower activity in high grade NHL (RR 10-15%) Redman et al. JCO 10:790, 1992
Fludarabine combination in LGBC lymphomasFMD regimen Previously Treated Recurrent/refractory (N=51) FMD protocol Fludarabine 25mg/m2 D1,2,3 Mitoxantrone 10mg/m2 D1 Dexamethasone 20mg D1-5 Recycle every 4 weeks x 8 • Response rate 94% • CR 47% • Response duration 21 mons of CR Mclaughlin et al. JCO 14: 1262, 2996
Number : 381 cases Immediately treated : 248 Treatment after W/W : 133 Phase III study Marcus et al. Ann Oncol 13; (suppl2): abs#181, 2002 Fludarabine x 8CVPx 8 68% ORR 51% 38% CR 15% 21mon TTP 15mon 68% 5 years 60% (NS) survival P = 0.001
Number : 381 Immediately treated : 248 Treatment after W/W : 133 Adverse Events Fludarabine CVP 28% Neutropenia (Gr III/IV) 12% (p<0.005) 8% Thrombo (Gr III/IV) 1% (p<0.01) 2% Infection 3% Alopecia more significant Marcus et al. Ann Oncol 13; (suppl2): abs#181, 2002
FM compared to CHOP in follicular lymphoma (BCL2 +ve BM/PB) FM X 6 CHOP x 6 72 Number 68 68% CR 42% 39% Molec CR 19% P=0.003 P=0.001 Zinzani et al. JCO 2004 (july)
FM CHOP (n=68) (n=72) Grade 3-4 toxicity No. Pts % No. Pts % p Neutropenia 22 30 27 39 n.s. Nausea/vomiting 2 3 15 22 0.000 Alopecia 10 14 58 85 0.000 Peripheral Neurologic Toxicity 0 / 18 26 0.000 Constipation 0 / 22 32 0.000 Toxicity of chemotherapy Zinzani et al, JCO 2004
PROS More quickly active Active on a minor large cell population ? CONS Cardiac toxicity Alopecia Hampers salvage treatments No beneficial effect of CHOP vs regimens without adriamycin in Terms of OS Up-front Anthracycline: why and why not? CHOP is not a standard first-line regimen forlow grade lymphoma. Adriamycin is an important drug for : - relapses - histological transformations
Fludarabine may induce unique toxicities Fludarabine is both myelotoxic and lymphotoxic leading to marked immuno suppression susceptibility to opportunistic infections (reduction of CD4 T helper cells is seen up to 1 year of discontinuation of the drug) Wijermans et al. Eur J hematology; 50: 292, 1993
Fludarabine may induceunique toxicities including: • Stem cell depletion • Hemolytic anemia • Neurotoxicity • Pulmonary toxicity • Hearing loss • Renal impairment
Effect of up-front Anthracycline and Purine analogueon risk of transformation • Retrospective review of 260 patients J Clin Oncol 2006; 24:Abstract 7510.
Low Grade B Cell Lymphoma Fludarabine • Currently available data do not recommend the use of this agent as first line outside controlled clinical studies except in CLL and SLL
Low Grade B Cell Lymphoma Fludarabine • In cases with small lymphocytic lymphoma (as in CLL) there is a good reason to use first line Fludarabine in combination with Cyclophosphamide with or without Mitoxantrone. • Also in patients with Lymphoplasmacytic Lymphoma and macroglobuliaemia ,Fludarabine usually in combination with Cyclophosphamide may be considered in front line management. • In Hairy cell leukemia treatment with another purine analog (2CDA) is considered as the standard of care in this disease. Of notice , 85% of the treated patients achieve very durable remissions with only 2 courses of 2CDA
FLUDARABINE IN W M FLUDARABINE CAP N=46 N=46 OR 30% 11% p=0.019 MRD 19Ms 3Ms p<0.01 Leblond el al Blood,2001
Bendamustine • Bendamustine is a novel nitrogen mustard and antimetabolite hybrid which is noncross-resistant with other alkylating agents. • This drug has been extensively used in East Germany for over 40 years with activity in NHL, chronic lymphocytic leukemia, and multiple myeloma, with an acceptable safety profile. During the last few years, the drug was made available in other countries
Bendamustine • Bendamustine was found to be one of the most promising agents in the treatment of B cell NHL. • Around 70% of patients with relapsed/refractory low grade B cell NHL and mantle cell lymphoma respond to Bendamustine as single agent, ( including 15-30% CRs), thus setting the new standard for drug activity in such patients Friedberg JW, Cohen P, Chen L et al. Bendamustine in patients with rituximab-refractory indolent and transformed non-Hodgkin's lymphoma: Results from a phase II multicenter, single-agent study. J Clin Oncol 2008;26:204–210
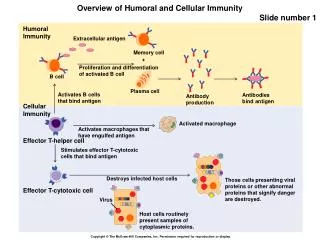
Target Antigens in Lymphoid Malignancies • Many cell-surface antigens are expressed on lymphoma cells which are virtually always expressed on their nonmalignant counterparts as well. • Therefore, the malignant B cells can be targeted and eradicated by specific antibodies directed against their surface antigens. • However surface antigens suitable for targeting should have certain features to allow effective and safe therapeutic use in the clinic. TCR Idiotype CD4/8 CD19 CD3 CD20 CD25 B cell T cell CD22 HLA-DR CD52 CD52 CD23
CD 20 as an Ideal Target for Immunotherapy of B cell Lymphomas • CD20 is a transmembrane surface antigen • involved in B cell growth and maturation • It is expressed only on B cells (precursor and mature) • BUT NOT on stem cells, normal mature plasma cells • or other normal tissues • It is expressed on more than 85% of B cell Lymphoma Tedder & Engel. Immunol Today;15 : 450, 1994 Anderson et al. Blood;63 : 1424, 1984
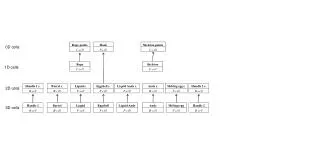
Hairy cell Large cell Burkitt’s lymphoma Marginal zone Follicular small cell Small cleaved LP/Waldenström’s Mantle cell CLL/PLL CLL CD20 expression in B-cell malignancies Histology 0 100 200 300 400 500 600 Mean channel fluorescence LP = lymphocyte predominantPLL = prolymphocytic leukaemia Adapted from Maloney GD. Semin Hematol 2000;37(4 Suppl. 7):17–26