Download
1 / 40
910 likes | 3.99k Vues
Management of Foreign body aspiration. Speaker : Dr. Pragati Nanda. Moderator : Dr. Subhash Chawla. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. FOREIGN BODY ASPIRATION. Common ,but a life threatening problem. Cause of morbidity and mortality.

E N D
Management of Foreign body aspiration. Speaker : Dr. Pragati Nanda. Moderator : Dr. Subhash Chawla. www.anaesthesia.co.inanaesthesia.co.in@gmail.com
FOREIGN BODY ASPIRATION • Common ,but a life threatening problem. • Cause of morbidity and mortality. • Can cause chronic lung injury. • Challanging for anaesthetist. • High degree of suspicion is required for diagnosis.
Foreign Bodies • Foreign body aspiration • Toddlers • Oral exploration • Lack posterior dentition • Easy distractibility • Cognitive development (edible?)
Involuntary safety muscular mechanics in adults. • 1. soft palate is pulled up and posteriorly,prevent reflux of food into nasal cavities. 2. palatopharangeal folds move medially to form a slit, allow only chewed food to pass. 3. epiglottis moves down and close to glottis.
Foreign Body Aspiration • Vegetable matter in 70-80% • Peanuts & other nuts (35%) • Carrot pieces, beans, sunflower & watermelon seeds • Metallic objects • Plastic objects
Organic f.b are more liable to evoke larangospasm, tracheobronchitis and lung infection. Hence, when patient presents, often has fever. • vegitable FB are slippery,hard to grip and friable. They usually get swollen, struk at subglottis, may lead to complete obstruction.
PATHOPHISIOLOGY • Bronchi – 80-90% • Right mainstem most common • Carina • Less divergent angle • Greater diameter • Trachea • Larynx • Larger objects, irregular edges • Conforming objects
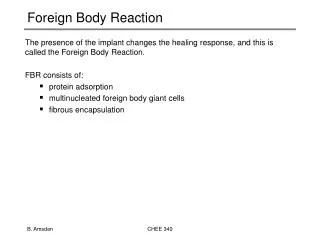
Relevant Anatomy • Airway foreign bodies can become lodged in the larynx, trachea, and bronchus. The size and shape of the object determine the site of obstruction. • large, round, or expandable objects produce complete obstruction, and irregularly shaped objects allow air passage around the object, resulting in partial obstruction.
TYPES OF OBSTRUCTION. • 1. check valve: air can be inhaled but not exhaled.[emphysema]. 2. ball valve: air can be exhaled but not inhaled.[broncho pul segment collapse]. 3. bypass valve: FB partially obstructs both in insp. and exp. 4. stop valve: total obstruction, airway collapse and consolidation.
Presentation • In general, aspiration of foreign bodies produces the following 3 phases: • Initial phase - Choking and gasping, coughing, or airway obstruction at the time of aspiration • Asymptomatic phase - Subsequent lodging of the object with relaxation of reflexes that often results in a reduction or cessation of symptoms, lasting hours to weeks • Complications phase - Foreign body producing erosion or obstruction leading to pneumonia, atelectasis, or abscess
Foreign Body Aspiration • History • Choking • Gagging • Wheezing • Hoarseness • Dysphonia • Can mimic asthma, croup, pneumonia • “A positive history must never be ignored, while a negative history may be misleading”
Foreign Body Aspiration • Tachepnia, rib and sternal retraction, cyanosis,n/v. • Hypoxic seizures, arrest,hypoxic brain damage. • Asymptomatic interval • 20-50% not detected for one week • Inflammation and Complications • Cough • Emphysema • Obstructive atelectasis • Hemoptysis • Pneumonia • Lung abscess • Fever
Foreign Body Aspiration • Physical exam • Larynx/cervical trachea • Inspiratory or biphasic stridor,aphonia, complete obstruction. • Intrathoracic trachea • Prolonged expiratory wheeze,comp obs. • Bronchi • Unequal breath sounds • Diagnostic triad - <50% • Unilateral wheeze • Cough • Ipsilaterally diminished breath sounds • Fiberoptic laryngoscopy
Foreign Body Aspiration • Radiography • PA & lateral views of chest & neck • Inspiration & expiration [atelectesis on insp, hyperinflation on exp. In affected bronchus.] • Lateral decubitus views [lower lung doesn’t collapse if FB present.] • Airway fluoroscopy [for intraop evaluation, to locate FB in lung periphery.] • 25% have normal radiography
X-RAY FINDINGS • Obstructive emphysema • Normal x-ray • Pneumonitis • Collapse with mediastinal shift • Foreign body. If still a diagnostic delima,CT scan is advised.
Indications • Perform surgical intervention with rigid bronchoscopy on patients: • who have a witnessed foreign body aspiration. • those with radiographic evidence of an airway foreign body. • those with the previously described classic signs and symptoms of foreign body aspiration. A strong history of suspected foreign body aspiration prompts an endoscopic evaluation, even if the clinical findings are not as conclusive or are not present
Contraindications • No contraindications exist to the removal of an airway foreign body from a child. • If necessary, health problems can be optimized before surgical intervention. However, even children who are at high risk due to health reasons still need surgical intervention to remove the foreign body.
History of the Procedure • Until the late 1800s, airway foreign body removal was performed by bronchotomy. • The first endoscopic removal of a foreign body occurred in 1897. • Chevalier Jackson revolutionized endoscopic foreign body removal in the early 1900s with principles and techniques still followed today. • The development of the rod-lens telescope in the 1970s and improvements in anesthetic techniques have made foreign body removal a much safer procedure.
Foreign Body Aspiration • Goal of treatment • Prompt endoscopic removal under conditions of maximal safety and minimal trauma. • GA is always technique of choice. • Communication and cooperation between anaesthetist and endoscopist is must.
ANAESTHETIC MANAGEMENT • Challanging; • Fighting irritable child. • Full stomach. • Sharing of airway. • Difficult to maintain oxygenation and ventilation,as pulmonary gas exchange is already reduced. • Difficulty pertaining to pediateric airway.
Usually NOT A DIRE EMERGENCY • Trained personnel • Instruments assembled and checked • Await for emptying of stomach • Find duplicate FB to test instruments and techniques
Preoperative considerations. • Severity of airway obstruction, gas exchange and level of conciousness. • Nature and location of FB,degree and duration of obstruction. • fasting status. Delaying intervention must be balanced against potential functional impairment and oxygenation. • metoclopramide 0.15mg/kg iv. • Atropine 0.02mg/kg iv.
Foreign Body Aspiration • General anesthesia • Spontaneous ventilation • Laryngoscopes • Bronchoscopes • Suction • Forceps • Rod-lens telescopes
GOALS OF ANAESTHESIA • 1. Adequate oxygenation. • 2. Controlled cardiorespiratory reflexes during bronchoscopy. • 3. Rapid return of airway reflexes. • 4. Prevention of pulmonary aspiration. • 5. Meticulous monitoring : spo2,ECG,NIBP,EtCO2.
TECHNIQUE • Oxygen sevoflurane induction. • Monitor, IV line. • Ketamine 2mg/kg- safe in peadtric pts,full stomach,leaves cough reflex intact,provides CVS stability and prevents bronchospasm. • Atropine 0.02mg/kg- dec secreations and obtund autonomic reflexes during airway instrumentation. • Nitrous oxide is avoided,as it inc gas volume,air traping and possible rupture of affected lung. • Suxa 1.5 mg/kg if controlled ventilation planned.
Foreign Body Aspiration • Ready to assume airway during induction • Laryngoscopy • Topical anesthesia- ligocaine spray 3-4mg/kg.[prevents larangospasm] • Examination of upper airway • Atraumatic insertion of bronchoscope • Bronchoscopy • Attached to ventilating circuit
Foreign Body Aspiration • Bronchoscopy • Suction opposite bronchus • IPPV through side arm mapelson F circuit. • Advance to foreign body • Atraumatically grasp foreign body • Repeat bronchoscopy • Suction bronchus • Multiple foreign bodies in 5-19% • Remove granulation tissue • Topical vasoconstrictors for bleeding
Foreign Body Aspiration • Slipped foreign body • Push back into bronchus,stablise and remove. • Sharp foreign body • Advance bronchoscope over FB, to prevent trauma.
Anaesthetic maintainence • oxygen, halo/iso.[ give more time for airway manipulation] Or rpt ketamine.[no OT pollution] • Suxa 0.25-0.5mg/kg with atropine 0.02mg/kg. • High flows are needed to compensate leak around bronchoscope. • Ventilation has to be intrupted while suctioning and removal of foreign body. • If foreign body is big/swollen tracheostomy may be needed.
Big FB can be taken out in piecies. • Apnea/ oxygen insufflation, is prefered at some crucial time, ideally should not last beyond 1min. After 5 min hypercarbia may lead to dysarrythmias. • If ventilation is inadequate with rigid broncoscope,high frequency jet ventilation via bronchoscope or ECMO can be used. • For FB embeded in mucosa,wait for 48-72hrs. Let odema subside. Rpt bronchoscopy , if unsuccessful- thoracotomy.
Spontaneous v/s controlled ventilation • SPONTANEOUS VENTILATION. ADV; 1. no dislodgement of FB. 2. unhurried bronchoscopy. 3. relatively safe. DISADV; 1. inc coughing, bucking. 2. inc chances of bronco/ larangospasms and arrythmias.[inadequate depth]. 3. inc resistance bcoz of bronchoscope and suctioning. 4. large FB doesn’t come out because of VC movements and closure.
After removal of foreign body, check bronchoscopy is done to ensure full clearence and check impaction site for trauma/ bleeding/granulation. • Inj Dexamethasone 0.4-1mg/kg, humidified oxygen and bronchodialators given postop.
Foreign Body Aspiration • Complications • Larago/bronchospasm; ms. Relaxation,adequate ventilation. • Arrhythmias: hyperventilation , lignocaine. • Pneumothorax • Pneumomediastinum • Pneumonia • Antibiotics, physiotherapy • Atelectasis • Expectant management, physiotherapy
If postop stridor or distress: nebulise with racemic Epinephrine. • Observe the child in recovery room for signs of subglotic odema, haemorhage, bronchospasm and airway perforation. • Postop SPO2 and ECG monitoring. • 6-8hrs later chest x-ray to assess-lung expantion, exclude pneumothorax, residual FB,mediastinal emphysema from barotrauma.
THANKYOU. www.anaesthesia.co.inanaesthesia.co.in@gmail.com