Download
1 / 31

E N D
1. Scabies and pediculosis Ziad Elnasser, MD, Ph.D
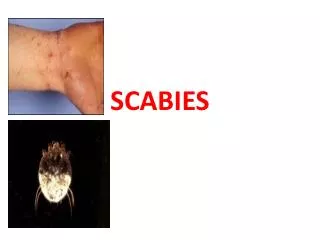
2. Scabies Sarcoptes scabiei or the itch mite.
Burrows resides in human skin.
Eggs, Larvae, adult (Incomplete metamorphoses)
Arachnid, 4 pairs of legs, 0.35mm.
6. Epidemiology Worldwide, Sexual promiscuity, poverty, poor hygiene overcrowding, and malnutrition.
Intimate personal contact, casual contact or dust samples.
Extent of clinical manifestation is related to level of cleanliness.
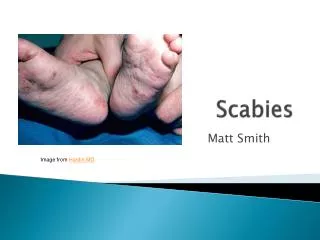
7. Clinical manifestations Intense itching especially at night.
Erythematous papules, excoriations and occasionally vesicles.
Interdigital web spaces, wrists, axillary folds, periumbilical skin, pelvic girdle, penis and ankles.
Classic linear burrows.
11. Diagnosis Clinical presentation.
Skin scraping and demonstration of the
mite microscopically.
12. Complications Secondary impetiginization.
Eczematous eruption.
Scabies incognito if corticosteroids are used.
Delayed hypersensitivity reaction.
13. Norwegian scabies Severe variant.
Institutionalized persons, down syndrome, and AIDS patients.
Hyperkeratotic crusted nodules.
Secondary bacterial infections, septicemia and death.
14. Treatment 1% solution of Lindane not for infants, pregnant women or after a bath.
5 % cream Permethrin safer.
6% � 10% precipitated sulfur in petrolium daily for 3 days.
Antipruritic drugs.
Treat secondary infections.
Ivermectin in severe cases.
Treat all contacts and linen.
15. prevention Gloves.
Prophylactic treatment for close contacts.
Isolation and the use of disposable items.
16. Pthirus pubis Crab louse.
Could be found other than genital region.
2mm in length, powerful legs, hair attachment, moves slowly.
Incomplete metamorphosis, eggs, nymph and adult.
Eggs operculated, shiny, stick to hair (nits)
21. Clinical manifestations Pruritis.
Maculopapular rash.
Excoriation.
Eye lashes scaling.
Skin thickening, macular swellings, hyperpigmentations, Subcutaneous hemorrages (Vagabond�s disease).
23. Diagnosis Clinical manifestation.
Nits, nymphs or adult louse.
24. Treatment Lindane.
Permethrin.
Antipruritic drugs.
25. Gardnerella vaginalis Hemophilus vaginalis, Corynebacterium vaginalis.
Gram variable, although amino acids and fatty acids analysis shows gram positive, oxidase and catalase negative
Enriched media, beta hemolytic colonies on human blood.
Endotoxin but no lipid A.
26. Epidemiology 69% presence in the vagina.
No signs or symptoms.
100% Bacterial vaginosis, male urethra.
28. Pathogenesis Pili and adherence to McCoy cells.
Hemolysin (Cytolytic toxin).
Normal flora with phospholipase activity.
Associated with premature rupture of the membranes.
Serum resistant.
29. Clinical manifestations Bacterial vaginosis:
Present with mixed anaerobic flora.
Predispose to bacterial vaginitis.
Fishy odor discharge.
Vulvar burning or pruritis.
Gram stain of vaginal fluid rather than by culture.
Urinary tract infection: Infrequent, difficult to diagnose.
Bacteremia: obstetrics events.
Neonatal infection.
30. Diagnosis Small pinpoint colonies.
Beta hemolysis on human blood.
Blood culture in SPS free bottles.
Catalase and oxidase neg, Na hippurate positive.
31. Treatment Penicillin.
Ampicillin
Gentamycin.
Metronidazole.
Clindamycin.