Download
1 / 30
350 likes | 431 Vues
Thrombocytopenia. January 2018 Jason aboudi mouabbi MD. Definition. Mild: 100 to 150 Moderate : 3 0 to 100 Severe : < 3 0 Keep in mind, these are 95% confidence intervals, so 2.5% of population < 150. Pathophysiology. Four Main Categories Redistribution Hemodilution

E N D
Thrombocytopenia January 2018 Jason aboudimouabbi MD
Definition • Mild: 100 to 150 • Moderate: 30 to 100 • Severe: < 30 Keep in mind, these are 95% confidence intervals, so 2.5% of population < 150
Pathophysiology Four Main Categories • Redistribution • Hemodilution • Bone Marrow Dysfunction • Platelet Destruction/Consumption
Let’s Start! • Redistribution • Spleen carries ⅓ of our total body platelet mass • Hypersplenism redistributes this higher (ex: ½) • Hemodilution • Platelet-poor transfusions (PRBC, fluids)
Easy, right? • Bone Marrow Dysfunction • MDS • Leukemia • Paroxysmal Nocturnal Hemoglobinuria • Infection • Alcoholism • Nutritional Deficits • ITP (decreased BM production and peripheral destruction) • Malignancy (extension into BM)
Bone Marrow • Leukemia • Leukemic cells inhibit cell differentiation • PNH • Link with aplastic anemia and bone marrow failure • Complement mediated damage to three cell lines • Alcoholism • Hypersplenism and Vitamin deficiency • Direct megakaryocyte toxicity • Decreased TPO production
Bone Marrow • Myelodysplastic Syndromes • Dysplastic and ineffective blood cell production • Diagnosis • Cytopenia (not just platelets) • Peripheral/BM smear showing dysplasia • Tear drop cells • Smudge cells • Hypersegmented neutrophils • Dohle bodies • Giant platelets • Treatment • Mainly bone marrow transplantation
Bone Marrow • Infection • Viral • HIV • ITP-like syndrome • Direct megakaryocyte toxicity • Hepatitis C, MMR vaccine and EBV • Bacterial + Parasites • BM suppression or DIC in sepsis • H. pylori, leptospirosis, malaria, babesiosis
Destruction/Consumption • Almost always antibody mediated Remember This: • Thrombotic Microangiopathies • A group of diseases that are associated with thrombosis in arterioles • Includes TTP-HUS and DIC among others We will discuss • Immune Thrombocytopenia • Drug-Induced Thrombocytopenia • Evan’s Syndrome • Heparin Induced Thrombocytopenia • TTP-HUS • DIC
Immune Thrombocytopenia • Pathophysiology • Inciting event causing autoantibody formation • Malignancy (CLL) • Rheumatological diseases (SLE, APS, Evan’s) • Viral/Bacterial infections • HIV, Hep C, CMV, VZV • Sometimes H. pylori, Gram - bacteria and LPS • Molecular mimicry to Gp2b3a receptor on platelets
Immune Thrombocytopenia • Diagnosis of exclusion! • Treatment • Plt < 20 and bleeding? • Transfuse with IVIG and/or Steroids • Plt > 30 and no bleeding? • No need for treatment • Treatment Regimens • Utilize steroids first, usually cheaper, faster and the correct answer on the board!(Prednisone 1 mg/kg/day) • IVIG 1 g/kg/day x 2 days • Rituximab or Splenectomy if not responsive > 6 months
Drug Induced Thrombocytopenia (DIT) • Pathophysiology • Platelet Destruction • Medication induced change in antigen creating an autoantibody • Platelet Production • Megakaryocyte death or decreased production • Diagnosis • Initiation in about one week of drug start • Usually beta lactams, vancomycin, linezolid, rifampin, AEDs and Quinine • Treatment • Removal of the drug • Recovery should be in about one week as well
Evan’s Syndrome • Quick Introduction • Autoimmune-Hemolytic Anemia with associated thrombocytopenia • Look for other autoimmune diseases, such as SLE, CVID, HIV and HCV • Usually treat underlying cause or utilize steroids
Discussion So Far We will discuss • Immune Thrombocytopenia • Drug-Induced Thrombocytopenia • Evan’s Syndrome • Heparin Induced Thrombocytopenia • TTP-HUS • DIC
Heparin Induced Thrombocytopenia • Type 1 • Direct heparin effect, associated with platelet aggregation • Transient drop in 1-2 days, usually not < 100 • No need to stop Heparin • Type 2 • PF-4 complexed with Heparin causing autoantibodies • Heparin-Induced Antibodies • Autoantibodies without HIT clinical features
Heparin Induced Thrombocytopenia • Diagnosis: 4Tof HIT (high sensitivity and negative predictive value) • Thrombosis • venous more likely than arterial • Thrombocytopenia • 50% drop, usually not < 20 • Timing • Within 7 days, can be earlier with heparin exposure < 30 days ago • Alternate Causes?
Heparin Induced Thrombocytopenia • Labs • HIT-ELISA (tests for anti-PF4 antibodies) • Sensitivity 97% and Specificity 70% • If < 0.4 = unlikely, if > 2.0 = likely • Best to use if Intermediate to High 4T score • Serotonin Release Assay • Sensitivity + Specificity > 95% • Use if discordant results or indeterminate ELISA
Heparin Induced Thrombocytopenia • Treatment • Immediately start non-Heparin anticoagulant • Renal Dysfunction: Argatroban, Bivalirudin • Liver Dysfunction: Fondaparinux • Both? Use Argatroban • Long-Term, when Plts > 150 • No Thrombosis: Warfarin x 3 months • Thrombosis: Warfarin > 6 months • Remember: educate patient on Heparin allergy
Thrombotic Microangiopathies • Includes TTP, HUS, aHUSand DIC • Other etiologies that we won’t discuss at this time (TTP-like diseases): • Cyclosporine or Tacrolimus (causing platelet aggregation) • Malignancy (via entities that resemble TTP-HUS) • Antiphospholipid Antibody (resembles TTP-HUS) • SLE (can occur without antiphospholipid antibodies)
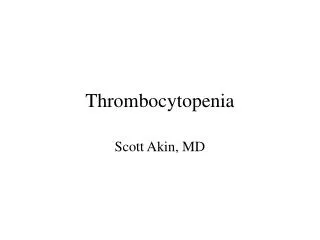
Blood Flow With ADAMTS13 No ADAMTS13 ???? A D A M T S 1 3 Endothelium Thrombotic Thrombocytopenic Purpura TTP Platelet Normal vWF multimer Ultralrge vWF multimer Erythrocyte Schistocyte Tissue ischemia
TTP • Diagnosis • ADAMTS13 activity less than 10% However this test take ~1 week to come back!!! • Historically the TTP Pentad was used (Fever, AMS, Renal Failure, Thrombocytopenia and schistocytes) • This was proved to be very unreliable
TTP Treatment • Urgent Plasmapheresis (PLEX)with steroids • Consult Hematology + Nephrology • Extremely complicated to manage
HUS: STEC-HUS and aHUS • Causes: • STEC-HUS: E.coli H7:0157 producing shiga toxin (Verotoxin) that lead to overwhelming activation of the complement system • aHUS: Chronic uncontrolled activation of the complement system due to acquired mutations in the complement regulatory proteins (factor H, factor I, or membrane cofactor protein) • Epidemiology: • STEC-HUS: Primarily affect children under the age of 5 • aHUS: Can occur at any age. • Clinical: • Prodrome of abdominal pain, vomiting and bloody diarrhea in STEC-HUS only • HUS triad: Hemolytic anemia, thrombocytopenia and renal failure • Late presentation: Lethargy and seizure • Treatment: • Mainly Supportive • NO antibiotics • NO PLEX • Eculizumab in severe cases
ECULIZUMAB (SOLIRIS) Monoclonal Ab against C5 leading to inability to form the MAC complex However the MAC complex is vital to help against encapsulated organisms especially meningococcal infections. Due to the increased risk of meningococcal infections, meningococcal vaccination is recommended at least 2 weeks prior to receiving eculizumab, unless the risks of delaying eculizumab therapy outweigh the risk of developing a meningococcal infection, in which case the meningococcal vaccine should be administered as soon as possible.
Disseminated Intravascular Coagulation • Acute versus Chronic • Acute(usually due to sepsis, trauma, AML) • procoagulation causing consumption that liver production can’t keep up with • FSP also inhibits coagulation • Leading to significant bleeding • Chronic(usually malignancy) • Procoagulation which is constant and production = consumption • FSP do not build up • Usually thrombosis and not bleeding
Disseminated Intravascular Coagulation • Diagnosis • Clinical Findings (bleeding/thrombosis) + Labs • Low Fibrinogen, and platelets • High PT/PTT and D-Dimer • DIC Score: • Treatment • Plt transfusion if < 10 or < 50 and bleeding • FFP if PT, PTT increased and Fibrinogen normal • Cryo if PT, PTT normal and Fibirinogen low
TAKE HOME POINTS • Thrombocytopenia can be from four different categories: • Redistribution • Hemodilution • Bone Marrow Dysfunction • Platelet Destruction/Consumption • A majority will be Platelet Destruction/Consumption • ITP has to be diagnosis of exclusion • DIT has a long list of medications that can cause them • HIT has the 4T clinical criteria and requires immediate anticoagulation • TTP-HUS is a medical emergency that should warrant a nephrology + hematology consult • DIC can be acute or chronic with the treatment being fixing the underlying cause
TAKE HOME POINTS • When should we transfuse platelets? • Significant bleeding? Goal > 50 • Invasive procedures needed? Goal > 50 • Neurosurgery or other high-risk procedures? Goal > 100 • Risk for spontaneous bleeding? Goal > 10
Thank you! As always you are welcome to download this lecture and other hematology/oncology lectures from our website www.mihemeonc.org