Download
1 / 67
670 likes | 724 Vues
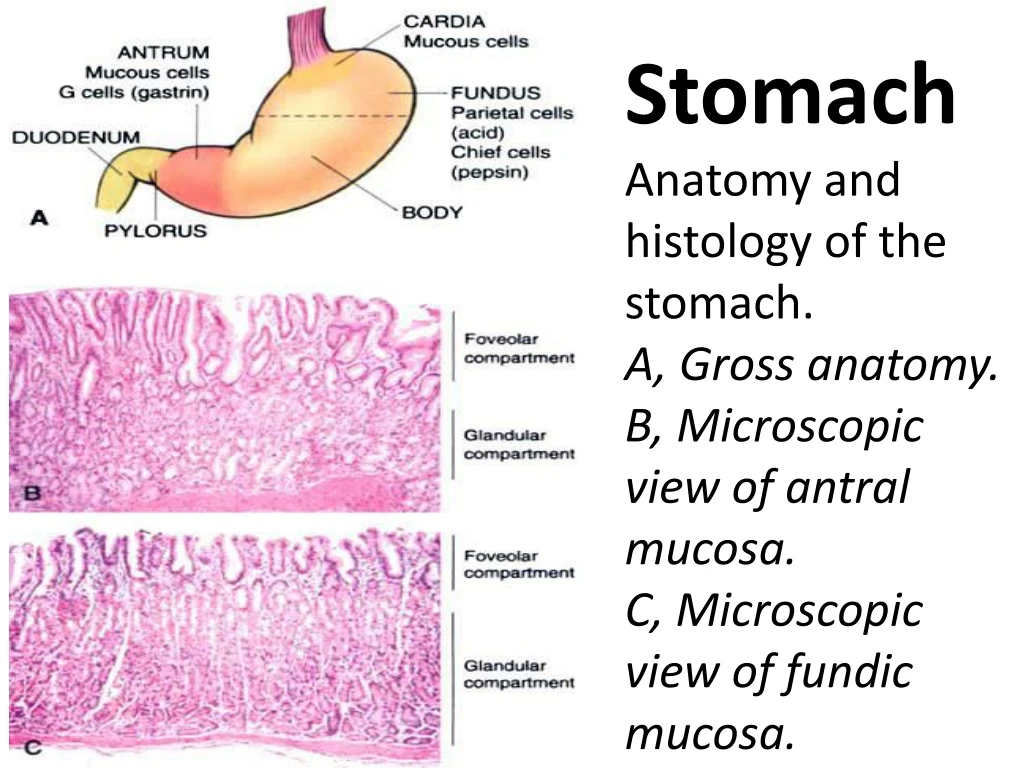
Stomach Anatomy and histology of the stomach. A, Gross anatomy. B, Microscopic view of antral mucosa. C, Microscopic view of fundic mucosa. Gastric disorders frequently cause clinical disease, ranging from bland chronic gastritis to gastric carcinoma.

E N D
StomachAnatomy and histology of the stomach. A, Gross anatomy. B, Microscopic view of antral mucosa. C, Microscopic view of fundic mucosa.
Gastric disorders frequently cause clinical disease, ranging from bland chronic gastritis to gastric carcinoma. Gastric infection with Helicobacter pylorirepresents the most common gastrointestinal infection. Occasionally, congenital anomalies are encountered; Congenital Gastric Anomalies 1. Pyloric stenosis : 1 in 300-900 live births ,Male-to-female ratio 3:1 Pathology: muscular hypertrophy of pyloric smooth muscle wall, the Symptoms: persistent, nonbilious projectile vomiting in young infant
2. Diaphragmatic hernia, Rare condition, Pathology: herniation of stomach and other abdominal contents into thorax through a diaphragmatic defect Symptoms: acute respiratory distress in newborn 3. Gastric heterotopia ,Uncommon Pathology: a nidus of gastric mucosa in the esophagus or small intestine ("ectopic rest") Symptoms: asymptomatic, or an anomalous peptic ulcer in adult
Gastric disorders give rise to symptoms similar to esophageal disorders, primarily heartburn and vague epigastric pain. With breach of the gastric mucosa and bleeding, hematemesisormelenamay ensue. Unlike esophageal bleeding, however, blood quickly congeals and turns brown in the acid environment of the stomach lumen. Vomited blood hence has the appearance of coffee
GASTRITIS This diagnosis is both overused and often missed-overused when it is applied loosely to any transient upper abdominal complaint in the absence of validating evidence, and missed because most persons with chronic gastritis are asymptomatic. Gastritis is simply defined as inflammation of the gastric mucosa. By far the majority of cases are chronic gastritis, but occasionally, distinct forms of acute gastritisare encountered.
Chronic Gastritis Chronic gastritis is defined as the presence of chronic inflammatory changes in the mucosa leading eventually to mucosal atrophyand epithelial metaplasia. In the Western world, the prevalence of histologic changes indicative of chronic gastritis is higher than 50% in the later decades of life
Pathogenesis • By far the most important etiologic association is chronic infection by the bacillus H. pylori. • This organism is a worldwide pathogen that has the highest infection rates in developing countries. • American adults older than age 50 show prevalence rates approaching 50%. • In areas where the infection is endemic, it seems to be acquired in childhood and persists for decades. • Most individuals with the infection also have the associated gastritis but are asymptomatic.
Gastritis is often accompanied by infection with Helicobacter pylori. This small curved to spiral rod-shaped bacterium is found in the surface epithelial mucus of most patients with active gastritis. The rods are seen here with a methylene blue stain
Helicobacter pylori. A Steiner silver stain demonstrates the numerous darkly stained Helicobacter organisms along the luminal surface of the gastric epithelial cells. Notethat there is no tissue invasion by bacteria
H. pylori is a noninvasive, non-spore-forming, S-shaped gram-negative rod measuring approximately 3.5 μm × 0.5 μm. Although H. pylori does not invade the tissues, it induces an intense inflammatory and immune response. There is increased production of proinflammatory cytokines such as interleukin IL-1, IL-6, tumor necrosis factor, and, most notably, IL-8. IL-8 is produced by the mucosal epithelial cells, and it recruits and activates neutrophils.
Several bacterial gene products are involved in causing epithelial cell injury and induction of inflammation. • Epithelial injury is mostly caused by a vacuolating toxin called VacA, which is regulated by the cytotoxin-associated gene A (CagA). • In addition, H. pylori secretes a urease that breaks down urea to form toxic compounds such as ammonium chloride and monochloramine.
The organisms also elaborate phospholipases that damage surface epithelial cells. Bacterial proteases and phospholipases break down the glycoprotein-lipid complexes in the gastric mucus, thus weakening the first line of mucosal defense. H. pylori enhances gastric acid secretion and impairs duodenal bicarbonate production, thus reducing luminal pH in the duodenum
This altered milieu seems to favor gastric metaplasia (the presence of gastric epithelium) in the first part of the duodenum. Such metaplastic foci provide areas for H. pylori colonization. Several H. pylori proteins are immunogenic, and they evoke a robust immune response in the mucosa.
Suffice it to say that gastritis develops as a result of the combined influence of bacterial enzymes and toxins and release of noxious chemicals by the recruited neutrophils. After initial exposure to H. pylori, gastritis may develop in two patterns: • an antral-type with high acid production and higher risk for the development of duodenal ulcer, and
(2) a pangastritis with multifocal mucosal atrophy, with low acid secretion and increased risk for adenocarcinoma Persons with chronic gastritis and H. pylori usually improve symptomatically when treated with antibiotics and proton pump inhibitors. Improvement in the underlying chronic gastritis may take much longer. Relapses are associated with reappearance of this organism.
Other forms of chronic gastritis are much less common in the United States; Autoimmune gastritis, which represents no more than 10% of cases of chronic gastritis, results from the production ofauto antibodies to the gastric gland parietal cells, in particular to the acid-producing enzyme H+,K+-ATPase. The autoimmune injury leads to gland destruction and mucosal atrophy, with concomitant loss of acid and intrinsic factor production.
Chronic atrophic gastritis,autoantibody demonstrated here is anti-parietal cell antibody. The bright green immunofluorescence is seen in the paritetal cells of the gastric mucosa.
The resultant deficiency of intrinsic factor leads to pernicious anemia. This form of gastritis is seen most often in Scandinavia, in association with other autoimmune disorders such as Hashimoto thyroiditis and Addison disease. Morphology Regardless of the cause or histologic distribution of chronic gastritis, the inflammatory changes consist of a lymphocytic and plasma cell infiltrate in the lamina propria , occasionally accompanied by neutrophilic inflammation of the neck region of the mucosal pits.
The inflammation may be accompanied by variable gland loss and mucosal atrophy. When present, H. pylori organisms are found nestled within the mucus layer overlying the superficial mucosal epithelium. In the autoimmune variant, loss of parietal cells is particularly prominent. Two additional features are of note. Intestinal metaplasia refers to the replacement of gastric epithelium with columnar and goblet cells of intestinal variety.
Chronic gastritis, showing partial replacement of the gastric mucosal epithelium by intestinal metaplasia (upper left) and inflammation of the lamina propria (right) containing lymphocytes and plasma cells.
This is significant, because gastrointestinal-type carcinomas seem to arise from dysplasia of this metaplastic epithelium. Second, H. pylori-induced proliferation of lymphoid tissue within the gastric mucosa has been implicated as a precursor of gastric lymphoma.
Lymphoid hyperplasia of the stomach presenting as multiple small intramucosal nodules, with Multiple reactive germinal follicles are situated in the deep aspect of the gastric mucosa adjacent to the muscularis mucosae.
Acute Gastritis Acute gastritis is an acute mucosal inflammatory process, usually of a transient nature. The inflammation may be accompanied by hemorrhage into the mucosa and, in more severe circumstances, by sloughing of the superficial mucosal epithelium (erosion). This severe erosive form of the disease is an important cause of acute gastrointestinal bleeding.
Pathogenesis The pathogenesis is poorly understood, in part because normal mechanisms for gastric mucosal protection are not totally clear. Acute gastritis is frequently associated with: • Heavy use of nonsteroidal anti-inflammatory drugs (NSAIDs), particularly aspirin • Excessive alcohol consumption • Heavy smoking • Treatment with cancer chemotherapeutic drugs • Uremia • Systemic infections (e.g., salmonellosis) • Severe stress (e.g., trauma, burns, surgery) • Ischemia and shock • Suicide attempts with acids and alkali • Mechanical trauma (e.g., nasogastric intubation) • Reflux of bilious material after distal gastrectomy
Morphology Acute gastritis ranges from extremely localized (as occurs in NSAID-induced injury) to diffuse, and from superficial inflammation to involvement of the entire mucosal thickness with hemorrhage and focal erosions. Concurrent erosion and hemorrhage are readily visible by endoscopy and termed acute erosive gastritis. All variants are marked by mucosal edema and an inflammatory infiltrate of neutrophils and possibly by chronic inflammatory cells.
Regenerative replication of epithelial cells in the gastric pits is usually prominent. Provided that the noxious event is short lived, acute gastritis may disappear within days with complete restitution of the normal mucosa. Clinical Features Depending on the severity of the anatomic changes, acute gastritis may be entirely asymptomatic, may cause variable epigastric pain with nausea and vomiting, or may present as overt hematemesis,melena, and potentially fatal blood loss. Overall, it is one of the major causes of hematemesis, particularly in alcoholics
GASTRIC ULCERATION Ulcers of the alimentary tract are defined histologically as a breach in the mucosa that extends through the muscularis mucosae into the submucosa or deeper. This is to be contrasted to erosions, in which there is a breach in the epithelium of the mucosa only. Erosions may heal within days, whereas healing of ulcers takes much longer. Although ulcers may occur anywhere in the alimentary tract, by far, the most common are the peptic ulcers that occur in the duodenum and stomach.
Peptic Ulcers Peptic ulcers are chronic, most often solitary, lesions that occur in any portion of the gastrointestinal tract exposed to the aggressive action of acidic peptic juices. At least 98% of peptic ulcers are either in the first portion of the duodenum or in the stomach, in a ratio of about 4:1
Epidemiology Peptic ulcers are remitting, relapsing lesions that are most often diagnosed in middle-aged to older adults, but they may first become evident in young adult life. They often appear without obvious precipitating influences and may then heal after a period of weeks to months of active disease. Even with healing, however, the propensity to develop peptic ulcers remains, in part because of recurrent infection with H. pylori. The male/female ratio for duodenal ulcers is about 3:1.
Genetic or racial influences seem to have little or no role in the causation of peptic ulcers. Duodenal ulcers are more frequent in persons with alcoholic cirrhosis, chronic obstructive pulmonary disease, chronic renal failure, and hyperparathyroidism. With respect to the last two conditions, hypercalcemia, whatever its cause, stimulates gastrin production and therefore acid secretion
Pathogenesis Two conditions are key for the development of peptic ulcers: (1) H. pylori infection, which has a strong causal relationship with peptic ulcer development, and (2) mucosal exposure to gastric acid and pepsin. Nevertheless, many aspects of the pathogenesis of mucosal ulceration remain murky. It is best perhaps to consider that peptic ulcers are created by an imbalance between the gastroduodenal mucosal defenses and the damaging forces that overcome such defenses Both sides of the imbalance are considered
H. pyloriinfection is the most important condition in the pathogenesis of peptic ulcer. The infection is present in 70% to 90% of persons with duodenal ulcers and in about 70% of those with gastric ulcers. Furthermore, antibiotic treatment of H. pylori infection promotes healing of ulcers and tends to prevent their recurrence. Hence, much interest is focused on the possible mechanisms by which this tiny noninvasive spiral organism tips the balance of mucosal defenses. Only 10% to 20% of individuals worldwide who are infected with H. pylori actually develop peptic ulcer.
NSAIDs are the major cause of peptic ulcer disease in persons who do not have H. pylori infection. The gastroduodenal effects of NSAIDs range from acute erosive gastritis and acute gastric ulceration to peptic ulceration in 1% to 3% of users. Because NSAIDs are among the most commonly used medications, the magnitude of gastroduodenal toxicity caused by these agents is quite large. Risk factors for NSAID-induced gastroduodenal toxicity are increasing age, higher dose, and prolonged usage.
Thus, those who take these drugs for chronic rheumatic conditions are at particularly high risk. Suppression of mucosal prostaglandin synthesis, which increases secretion of hydrochloric acid and reduces bicarbonate and mucin production, is the key to NSAID-induced peptic ulceration. Loss of mucin degrades the mucosal barrier that normally prevents acid from reaching the epithelium. Synthesis of glutathione, a free-radical scavenger, is also reduced. Some NSAIDs can penetrate the gut mucosal cells as well. Whether coexisting H. pylori infection affects NSAID-induced ulceration is not entirely settled. *Other events may act alone or in concert with H. pylori and NSAIDs to promote peptic ulceration.
Morphology All peptic ulcers, whether gastric or duodenal, have an identical gross and microscopic appearance. By definition, they are defects in the mucosa that penetrate at least into the submucosa, and often into the muscularis propria or deeper. Most are round, sharply punched-out craters 2 to 4 cm in diameter; those in the duodenum tend to be smaller, and occasional gastric lesions are significantly larger. Favored sites are the anterior and posterior walls of the first portion of the duodenum and the lesser curvature of the stomach.
The location within the stomach is dictated by the extent of the associated gastritis: antral gastritis is most common, and the ulcer is often along the lesser curvature at the margin of the inflamed area. Occasional gastric ulcers occur on the greater curvature or anterior or posterior walls of the stomach, the very same locations of most ulcerative cancers.
Classically, the margins of the crater are perpendicular and there is some mild edema of the immediately adjacent mucosa, but unlike ulcerated cancers there is no significant elevation or beading of the edges. The surrounding mucosal folds may radiate like wheel spokes. The base of the crater appears remarkably clean, as a result of peptic digestion of the inflammatory exudate and necrotic tissue. Infrequently, an eroded artery is visible in the ulcer (usually associated with a history of significant bleeding)
The histologic appearance varies with the activity, chronicity, and degree of healing. In a chronic, open ulcer, four zones can be distinguished : • the base and margins have a thin layer of necrotic fibrinoid debris underlain by (2) a zone of active nonspecific inflammatory infiltration with neutrophils predominating, underlain by (3) granulation tissue, deep to which is (4) fibrous, collagenous scar that fans out widely from the margins of the ulcer.
Chronic gastritis is extremely common among persons with peptic ulcer disease, and H. pylori infection is almost always demonstrable in those persons with gastritis. Similarly, individuals with NSAID-associated peptic ulcers do not have gastritis unless there is coexistent H. pylori infection. This feature is helpful in distinguishing peptic ulcers from acute gastric ulceration, because gastritis in adjacent mucosa is generally absent in the latter condition.
Clinical Features Most peptic ulcers cause epigastric pain, often described as burning but a significant minority first come to light with complications such as hemorrhage or perforation. The pain tends to be worse at night and occurs usually 1 to 3 hours after meals during the day. Classically, the pain is relieved by alkalis or food, but there are many exceptions. Nausea, vomiting, bloating, belching, and significant weight loss (raising the specter of some hidden malignancy) are additional manifestations
Bleeding is the chief complication, occurring in as many as one-third of patients, and may be life-threatening. Perforation occurs in about 5% of patients but accounts for two-thirds of deaths from this disease in the United States. Obstruction of the pyloric channel is rare. Malignant transformation occurs in about 2% of patients, generally from ulcers in the pyloric channel, and is very rare with gastric ulcers. In the latter event, it is often difficult to exclude the possibility that carcinoma was present from the outset.
Acute Gastric Ulceration Focal, acutely developing gastric mucosal defects that may appear after severe physiologic stress are called stress ulcers. Generally, there are many lesions located mainly in the stomach and occasionally in the duodenum. Stress ulcers are most commonly encountered in these conditions: • Severe trauma, including major surgical procedures, sepsis, shock, or grave illness of any type • Chronic exposure to gastric irritant drugs, particularly NSAIDs and corticosteroids • Extensive burns (these ulcers are known as Curling ulcers) • Traumatic or surgical injury to the central nervous system or an intracerebral hemorrhage (called Cushing ulcers; carry high risk of perforation).
The pathogenesis of these lesions is uncertain and may vary with the setting. NSAID-induced ulcers are linked to decreased prostaglandin production. The systemic acidosis that can accompany severe trauma and burns may contribute to mucosal injury presumably by lowering the intracellular pH of mucosal cells already rendered hypoxic by impaired mucosal blood flow. With cranial lesions, direct stimulation of vagal nuclei by increased intracranial pressure may cause gastric acid hypersecretion, which is common in these patients.
Morphology Acute stress ulcers are usually circular and small (<1 cm in diameter). The ulcer base is frequently stained dark brown by the acid digestion of extruded blood. Unlike chronic peptic ulcers, acute stress ulcers are found anywhere in the stomach. They may occur singly, but more often there are several, located throughout the stomach and duodenum
Microscopically, acute stress ulcers are abrupt lesions, with essentially unremarkable adjacent mucosa. They range in depth from very superficial lesions (erosion) to deeper lesions that involve the entire mucosal thickness (true ulceration). The shallow erosions are, an extension of acute erosive gastritis. The deeper lesions comprise well-defined ulcerations but are not precursors of chronic peptic ulcers. Even the deeper lesions do not penetrate the muscularis propria.
GASTRIC TUMORS As with the remainder of the gastrointestinal tract, tumors arising from the mucosa predominate over mesenchymal tumors. Mucosal tumors are classified into polyps and carcinoma Gastric Polyps The term polyp is applied to any nodule or mass that projects above the level of the surrounding mucosa.
However, the use of the term polyp in the gastrointestinal tract is generally restricted to mass lesions arising in the mucosa. Gastric polyps are uncommon and are found in about 0.4% of adult autopsies, as compared with colonic polyps, which are seen in 25% to 50% of older persons. In the stomach, these lesions are most frequently • hyperplastic polyps (80% to 85%), (2) fundic gland polyps (∼10%), and (3) adenomatous polyps (∼5%).
Morphology Hyperplastic polyps arise from an exuberant reparative response to chronic mucosal damage and hence are composed of a hyperplastic mucosal epithelium and an inflamed edematous stroma. They are not true neoplasms. Fundic gland polyps are small collections of dilated corpus-type glands thought to be small hamartomas. On the other hand, the less common adenomas contain dysplastic epithelium,adenomas are true neoplasms.
Gastric Carcinoma Among the malignant tumors that occur in the stomach, carcinoma is the most important and the most common (90% to 95%). Next in order of frequency are lymphomas (4%), carcinoids (3%), and stromal tumors (2%).
Epidemiology Gastric carcinoma is the second leading cause of cancer-related deaths in the world, with a widely varying geographic incidence. Japan and South Korea have the highest incidence (eight to nine times higher than in the United States and Western Europe),