Download
1 / 80
800 likes | 892 Vues
HERPESVIRUSES. Department of Pathogenic Biology Tongji Medical of College. Classification of Human Herpesviruses. Properties of herpesviruses. Structure & Composition Herpesvirus Culture Herpesviruses infection in host cell

E N D
HERPESVIRUSES Department of Pathogenic Biology Tongji Medical of College
Properties of herpesviruses • Structure & Composition • Herpesvirus Culture • Herpesviruses infection in host cell • The development of specific cell-mediated immunity seems important in recovery from the infections of herpesvirus
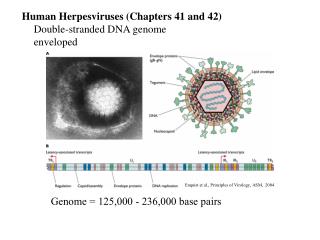
Structure & Composition double stranded DNA Size: 150-200nm Envelope: Present; associated glycoproteins. Capsid: Icosahedral, 95-105nm diameter; 162 hexagonal capsomers. Core: DNA around protein Genome: Linear, d/s DNA, 105-235kbp
Herpesvirus Culture • Herpes viruses can replicate in human diploid cells (human embryonic tissue) • produce cytopathic effect(CPE) • intranuclear acidophilic inclusion bodies • Multinucleated giant cells
Herpesviruses infection in host cell • Primary infections • Latent infection • Recurrent infections (reactivations)
Herpes Simplex Viruses • HSV-1 • HSV-2
Properties • Belong to the alphaherpesvirus subfamily of herpesviruses • ds DNA enveloped virus with a genome of around 150 kb • The genome of HSV-1 and HSV-2 share 50 - 70% homology. • They also share several cross-reactive epitopes with each other. There is also antigenic cross-reaction with VZV. • Man is the only natural host for HSV.
Glycoprotein "spikes" on the HSV surface. Between the capsid and the envelope is an ill-defined layer of proteins, collectively known as the tegument.
Epidemiology • HSV is spread by contact, as the virus is shed in saliva, tears, genital and other secretions. • By far the most common form of infection results from a kiss given to a child or adult from a person shedding the virus. • Primary infection is usually trivial or subclinical in most individuals. It is a disease mainly of very young children ie. those below 5 years.
Generally HSV-1 causes infection above the belt and HSV-2 below the belt. • Following primary infection, 45% of orally infected individuals and 60% of patients with genital herpes will experience recurrences. • The actual frequency of recurrences varies widely between individuals.
Pathogenesis • During the primary infection, HSV spreads locally and a short-lived viraemia occurs, whereby the virus is disseminated in the body. Spread to the to craniospinal ganglia occurs. • The virus then establishes latency in the craniospinal ganglia.
The exact mechanism of latency is not known, it may be true latency where there is no viral replication or viral persistence where there is a low level of viral replication. • Reactivation - It is well known that many triggers can provoke a recurrence. These include physical or psychological stress, infection; especially pneumococcal and meningococcal, fever, irradiation; including sunlight, and menstruation.
Primary infection and latent infection Herpes simplex virus can set up a primary infection in the lips, move to the trigeminal ganglion where it can remain latent. Virus can subsequently reactivate, move to the original site of infection and result in cold sores.
DISEASES! cold sore Gingivostomatitis eczema herpeticum herpes whitlow Genital herpes
Neonatal Herpes • Neonatal Herpes infections can be acquired in utero, during birth or after birth. • The newborns appear to be unable to limit the replication and spread of HSV and have potensity to develop severe disease. • Three categories of disease: • A. lesions localized to the skin, eye, and mouth • B. encephalitis with or without localized skin lesions • C. disseminated disease involving multiple organs, including central nervous system.
A large proportion of survivors of neonatal HSV infection have residual disabilities. • Acyclovir should be promptly given in all suspected cases of neonatal HSV infection. • The only means of prevention is to offer caesarean section to mothers with florid genital HSV lesions.
Diagnostic Laboratory Tests • Virus Isolation and Identification • Polymerase Chain Rection • Serological Tests
Cytopathic Effect of HSV in cell culture: Note the ballooning of cells. (Linda Stannard, University of Cape Town, S.A.) Positive immunofluorescence test for HSV antigen in epithelial cell. (Virology Laboratory, New-Yale Haven Hospital)
Treatment • The viral DNA synthesis inhibitors, such as acyclovir have been proved effective against HSV infection . • These drugs inhibit herpesvirus replication and may suppress clinical manifestations. • For the latent HSV the antiviral drugs have no effect. The drug resistant strains may emerge.
Prevention • There is no effective vaccine yet. • The experimental vaccines: • viral envelope glycoprotein antigens, • synthetic peptides of the glycoprotein antigens, • purified glycoprotein antigens by expressed in recombinant system. Such vaccines may be useful in the prevention of primary infection.
Varicella-Zoster Virus • Biological properties: • VZV has only one serotype. • VZV has no animal reservoir. (also known as Herpes Zoster Virus, Human Herpes Virus-3)
Epidemiology • Primary varicella is an endemic disease. Varicella is one of the classic diseases of childhood, with the highest prevalence occurring in the 4 - 10 years old age group. • Varicella is highly communicable, with an attack rate of 90% in close contacts.
Pathogenesis • The virus is thought to gain entry via the respiratory tract and spreads shortly after to the lymphoid system. • After an incubation period of 14 days, the virus arrives at its main target organ, the skin.
Following the primary infection, the virus remains latent in the cerebral or posterior root ganglia. In 10 - 20% of individuals, a single recurrent infection occurs after several decades. • The virus reactivates in the ganglion and tracks down the sensory nerve to the area of the skin innervated by the nerve, producing a varicellaform rash in the distribution of a dermatome.
Cytopathic Effect of VZV Cytopathic Effect of VZV in cell culture: Note the ballooning of cells. (Coutesy of Linda Stannard, University of Cape Town, S.A.)
Varicella • Primary infection results in varicella (chicken-pox) • Incubation period of 14-21 days • Presents fever, lymphadadenopathy. a widespread vesicular rash. • The features are so characteristic that a diagnosis can usually be made on clinical grounds alone.
Complications are rare but occurs more frequently and with greater severity in adults and immunocompromised patients. • Most common complication is secondary bacterial infection of the vesicles. • Severe complications which may be life threatening include viral pneumonia, encephalititis, and haemorrhagic chickenpox.
Rash of Chickenpox(Varicella) chicken-pox Each spot starts as a 2-4 mm diameter red papule which develops an irregular outline (rose petal) as a small vesicle appears on the surface. This 'dew drop on a rose petal' appearance is very characteristic of chickenpox.
Zoster (Shingles) • The occurrence of painful vesicles along the course of a sensory nerve of the head or trunk is the common picture. • The disease usually starts with severe pain and it lasts from weeks to months, and post zoster neuralgia can be debilitating. Within a few days, a crops of vesicles appears over the skin supplied by the affected nerves. • The head, neck and trunk are most often involved. • The duration and severity of the lesions are usually increased with advancing age.
Laboratory Diagnosis • The clinical presentations of varicella or zoster are so characteristic that laboratory confirmation is rarely required. • Laboratory diagnosis is required only for atypical presentations, particularly in the immunocompromised. • Virus Isolation • Direct detection - electron microscopy may be used for vesicle fluids but cannot distinguish between HSV and VZV. Immunofluorescense on skin scrappings can distinguish between the two. • Serology - the presence of VZV IgG is indicative of past infection and immunity. The presence of IgM is indicative of recent primary infection.
Treatment • Both varicella and zoster are usually mild, self-limited infection which require no therapy. • In contrast, varicella in neonates, immunocompromised patients, and some adults are potentially fatal, treatments attempt to be required.
There are a few antiviral drugs are effective against VZV, eg, acyclovir, valacyclovir, vidarabine, and interferons. • Acyclovir is useful in prevent the development of varicella and disseminated zoster in immunocompromised children and adults, but has no effect in prevent the posttherpetic neuralgia.
Prevention • An attenuated live-virus vaccine is widely applied in preventing varicella. • The vaccine is very effective in preventing varicella, but zoster still occurs in those previously infected persons, because the vaccine does not eliminate the latent state. • The vaccine virus can persists and is reactivated frequently; but recurrences are very mild. • Immunoglobulins contain high VZV specific antibody can be used to prevent the development of disease post-exposure to varicella in immunocompromised patients. Once the varicella started the immunoglobulins have no therapeutic value.
Cytomegalovirus • CMV is the pathogen of cytomegalic inclusion disease. It is asymptomatic. • it can be transmitted vertically or horizontally usually with little effect on the host. • Derives from the propensity for massive enlargement of cytomegalovirus infected cells.
Pathogenesis • Once infected, the virus remains in the person for life and my be reactivated from time to time, especially in immunocompromised individuals. • The virus may be transmitted in utero, perinatally, or postnatally. Perinatal transmission occurs. • Perinatal infection is acquired mainly through infected genital secretions, or breast milk. Perinatal infection is thought to be 10 times more common than congenital infection. • Postnatal infection mainly occurs through saliva. Sexual transmission may occur as well as through blood and blood products and transplanted organ.
Congenital Infection • Defined as the isolation of CMV from the saliva or urine within 3 weeks of birth. • Commonest congenital viral infection, affects 0.3 - 1% of all live births. The second most common cause of mental handicap after Down's syndrome and is responsible for more cases of congenital damage than rubella.
Transmission to the fetus may occur following primary or recurrent CMV infection. 40% chance of transmission to the fetus following a primary infection. • May be transmitted to the fetus during all stages of pregnancy. • No evidence of teratogenecity, damage to the fetus results from destruction of target cells once they are formed.
Perinatal infection • Infected maternal genital tract secretions • Breast-feeding • Perinatal Infected babies receive the antibodies from mothers, and perinatal Infections can be subclinical.
Blood Transfusion • Blood transfusion-acquired CMV infections in newborns. • the clinic phenomena will vary according to the amount of virus received and the serologic status of the blood donor.
Immunocompromised Hosts • The individuals who are at high risk for CMV disease include organ transplant recipients, patients with malignant tumors undergoing chemotherapy, and AIDS patients. • Pneumonia is the most common disease. • CMV can disrupt cellular processes with potential to promote malignant growth.
Immunity • IgM: during the primary infection ,persist for 3 or 4 months. • IgG: primary infection , persist lifelong. • Reactivation of latent infection occurs in the presence of humoral immunity. The presence of antibody in breast milk doesn’t prevent transmission of infection to breast-feeding infants.
immunocompromised patients who fail to develop IgM run a high risk of developing disseminated infection. Seroconversion determined by appropriate tests distinguishes primary from recurrent infection. • Cell-mediated immunity depressed with primary infection, and this may contribute to the persistent viral infection.
Diagnostic Laboratory Tests • Virus Isolation • Cell culture • Histopathology • Immunofluorescent Assay • Electron microscopy (EM) • ELISAs for CMV antigen in the urine • Detection of CMV DNA by PCR • CMV antigenaemia test Treatment Treatment