Download
1 / 1
10 likes | 143 Vues
What’s the Hype About Hyperoxaluria ?. Kirsten Boestfleisch, Lindsay Edmonds, Lena Husnay , Sarah Johnson. What is Primary Hyperoxaluria ?. Diet Implications.

E N D
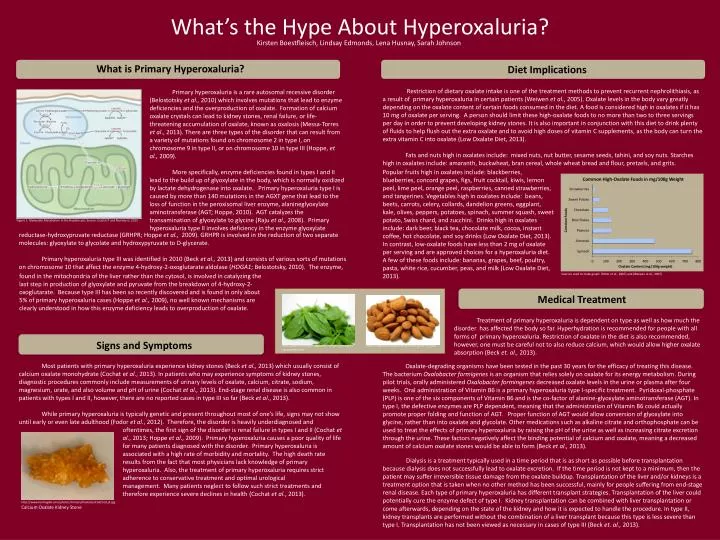
What’s the Hype About Hyperoxaluria? Kirsten Boestfleisch, Lindsay Edmonds, Lena Husnay, Sarah Johnson What is Primary Hyperoxaluria? Diet Implications Restriction of dietary oxalate intake is one of the treatment methods to prevent recurrent nephrolithiasis, as a result of primary hyperoxaluria in certain patients (Weiwenet al., 2005). Oxalate levels in the body vary greatly depending on the oxalate content of certain foods consumed in the diet. A food is considered high in oxalates if it has 10 mg of oxalate per serving. A person should limit these high-oxalate foods to no more than two to three servings per day in order to prevent developing kidney stones. It is also important in conjunction with this diet to drink plenty of fluids to help flush out the extra oxalate and to avoid high doses of vitamin C supplements, as the body can turn the extra vitamin C into oxalate (Low Oxalate Diet, 2013). Fats and nuts high in oxalates include: mixed nuts, nut butter, sesame seeds, tahini, and soy nuts. Starches high in oxalates include: amaranth, buckwheat, bran cereal, whole wheat bread and flour, pretzels, and grits. Primary hyperoxaluria is a rare autosomal recessive disorder (Belostotskyet al., 2010) which involves mutations that lead to enzyme deficiencies and the overproduction of oxalate. Formation of calcium oxalate crystals can lead to kidney stones, renal failure, or life-threatening accumulation of oxalate, known as oxalosis (Messa-Torres et al., 2013). There are three types of the disorder that can result from a variety of mutations found on chromosome 2 in type I, on chromosome 9 in type II, or on chromosome 10 in type III (Hoppe, et al., 2009). More specifically, enzyme deficiencies found in types I and II lead to the build up of glyoxylate in the body, which is normally oxidized by lactate dehydrogenase into oxalate. Primary hyperoxaluria type I is caused by more than 140 mutations in the AGXT gene that lead to the loss of function in the peroxisomal liver enzyme, alanineglyoxylate aminotransferase (AGT; Hoppe, 2010). AGT catalyzes the transamination of glyoxylate to glycine (Rajuet al., 2008). Primary hyperoxaluria type II involves deficiency in the enzyme glyoxylate Popular fruits high in oxalates include: blackberries, blueberries, concord grapes, figs, fruit cocktail, kiwis, lemon peel, lime peel, orange peel, raspberries, canned strawberries, and tangerines. Vegetables high in oxalates include: beans, beets, carrots, celery, collards, dandelion greens, eggplant, kale, olives, peppers, potatoes, spinach, summer squash, sweet potato, Swiss chard, and zucchini. Drinks high in oxalates include: dark beer, black tea, chocolate milk, cocoa, instant coffee, hot chocolate, and soy drinks (Low Oxalate Diet, 2013). In contrast, low-oxalate foods have less than 2 mg of oxalate per serving and are approved choices for a hyperoxaluria diet. A few of these foods include: bananas, grapes, beef, poultry, pasta, white rice, cucumber, peas, and milk (Low Oxalate Diet, 2013). Figure 1. Glyoxylate Metabolism in the Hepatocyte; Source: Cochat P and Rumsby G, 2013 reductase-hydroxypruvatereductase (GRHPR; Hoppe et al., 2009). GRHPR is involved in the reduction of two separate molecules: glyoxylate to glycolate and hydroxypyruvate to D-glycerate. Primary hyperoxaluria type III was identified in 2010 (Beck et al., 2013) and consists of various sorts of mutations on chromosome 10 that affect the enzyme 4-hydroxy-2-oxoglutarate aldolase (HOGA1; Belostotsky, 2010). The enzyme, found in the mitochondria of the liver rather than the cytosol, is involved in catalyzing the last step in production of glyoxylate and pyruvate from the breakdown of 4-hydroxy-2-oxoglutarate. Because type III has been so recently discovered and is found in only about 5% of primary hyperoxaluria cases (Hoppe et al., 2009), no well known mechanisms are clearly understood in how this enzyme deficiency leads to overproduction of oxalate. Sources used to make graph: (Ritter et al., 2007) and (Weiwenet al., 2007) Medical Treatment Treatment of primary hyperoxaluria is dependent on type as well as how much the disorder has affected the body so far. Hyperhydration is recommended for people with all forms of primary hyperoxaluria. Restriction of oxalate in the diet is also recommended, however, one must be careful not to also reduce calcium, which would allow higher oxalate absorption (Beck et. al., 2013). Signs and Symptoms http://eatgoodfood.org/are-almonds-good-for-you/ http://www.everyday-vegetarian-recipes.com/cooki ng-spinach.html Most patients with primary hyperoxaluria experience kidney stones (Beck et al., 2013) which usually consist of calcium oxalate monohydrate (Cochat et al., 2013). In patients who may experience symptoms of kidney stones, diagnostic procedures commonly include measurements of urinary levels of oxalate, calcium, citrate, sodium, magnesium, urate, and also volume and pH of urine (Cochatet al., 2013). End-stage renal disease is also common in patients with types I and II, however, there are no reported cases in type III so far (Beck et al., 2013). While primary hyperoxaluria is typically genetic and present throughout most of one’s life, signs may not show until early or even late adulthood (Fodor et al., 2012). Therefore, the disorder is heavily underdiagnosed and Oxalate-degrading organisms have been tested in the past 30 years for the efficacy of treating this disease. The bacterium Oxalobacterformigenes is an organism that relies solely on oxalate for its energy metabolism. During pilot trials, orally administered Oxalobacterformingenesdecreased oxalate levels in the urine or plasma after four weeks. Oral administration of Vitamin B6 is a primary hyperoxaluria type I-specific treatment. Pyridoxal-phosphate (PLP) is one of the six components of Vitamin B6 and is the co-factor of alanine-glyoxylate aminotransferase (AGT). In type I, the defective enzymes are PLP dependent, meaning that the administration of Vitamin B6 could actually promote proper folding and function of AGT. Proper function of AGT would allow conversion of glyoxylate into glycine, rather than into oxalate and glycolate. Other medications such as alkaline citrate and orthophosphate can be used to treat the effects of primary hyperoxaluria by raising the pH of the urine as well as increasing citrate excretion through the urine. These factors negatively affect the binding potential of calcium and oxalate, meaning a decreased amount of calcium oxalate stones would be able to form (Beck et al., 2013). oftentimes, the first sign of the disorder is renal failure in types I and II (Cochatet al., 2013; Hoppe et al., 2009). Primary hyperoxaluria causes a poor quality of life for many patients diagnosed with the disorder. Primary hyperoxaluria is associated with a high rate of morbidity and mortality. The high death rate results from the fact that most physicians lack knowledge of primary hyperoxaluria. Also, the treatment of primary hyperoxaluria requires strict adherence to conservative treatment and optimal urological management. Many patients neglect to follow such strict treatments and therefore experience severe declines in health (Cochatet al., 2013). • Dialysis is a treatment typically used in a time period that is as short as possible before transplantation because dialysis does not successfully lead to oxalate excretion. If the time period is not kept to a minimum, then the patient may suffer irreversible tissue damage from the oxalate buildup. Transplantation of the liver and/or kidneys is a treatment option that is taken when no other method has been successful, mainly for people suffering from end-stage renal disease. Each type of primary hyperoxaluria has different transplant strategies. Transplantation of the liver could potentially cure the enzyme defect of type I. Kidney transplantation can be combined with liver transplantation or come afterwards, depending on the state of the kidney and how it is expected to handle the procedure. In type II, kidney transplants are performed without the combination of a liver transplant because this type is less severe than type I. Transplantation has not been viewed as necessary in cases of type III (Beck et. al., 2013). http://www.herringlab.com/photos/Urinary/Oxalates/Cod/Cod_B.jpg Calcium Oxalate Kidney Stone