Download
1 / 36
370 likes | 511 Vues
Case 4: Andy. History. You have known Andy as a patient for 15 years Andy is 65 years of age and a retired bus driver You have been treating him for BPH for 10 years

E N D
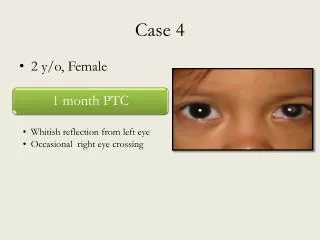
History • You have known Andy as a patient for 15 years • Andy is 65 years of age and a retired bus driver • You have been treating him for BPH for 10 years • At his last office visit almost a year ago, his IPSS score was 21 and he reported mixed satisfaction/dissatisfaction with his QoL related to urinary condition • Today Andy has made an urgent request to see you and presents with symptoms of severe LUTS • He has just filled-in his IPSS and QoL questionnaires and is quite distressed BPH = Benign Prostatic HyperplasiaIPSS = International Prostate Symptom ScoreQoL = Quality of LifeLUTS = Lower Urinary Tract Symptoms
Andy’s Response • Recognizing that Andy is distressed, you further inquire about his sleeping patterns and any outside stresses that could be affecting him. • You discover that he has to urinate at night so often that he is not getting any sleep • He has both severe irritative and obstructive symptoms • His wife is not speaking with him because she says he should have seen the Doctor sooner. He is now trying to get some sleep in the living room and has slept very poorly for the last 3 nights!
Andy’s Treatment History • Andy has previously been treated with α1-blocker therapy to which he has ceased to respond • Andy describes several similar acute episodes of pain over the past year, which got better after a few days.
How Would You Assess the Impact of Andy’s Urinary Problems on his Quality of Life?
IPSS = International Prostate Symptom ScoreAUA = American Urological Association
Discussion • The IPSS and Quality of Life due to Urinary Symptoms Questionnaires are requested of Andy • You ask him to complete the forms before proceeding • Here are Andy’s scores: International Prostate Symptom Score (IPSS) Patient name: Andy DOB: 06/08/40 ID: 0019-0024 Date of assessment: 29/06/05 Initial assessment (X) Monitor: during __X__ therapy after _____therapy/surgery
How Do You Interpret the Severity and Bother of Andy’s Symptoms?
Interpreting the IPSS and Bother Score • Andy’s IPSS = 32 (severe symptoms) • Andy’s Bother Score = 6 (terrible) IPSS = International Prostate Symptom Score
What Kind of Physical Examinations Would You Perform on Andy?
Results of the Physical Exam DRE = Digital Rectal Examination
Note • Andy has had severe burning when he voids but he has experienced no fever or chills • If he had fever or chills he should be admitted to the nearest emergency ward for monitoring and treatment in case of potential septicemia
Possible Diagnoses for Andy UTI = Urinary Tract InfectionBPH = Benign Prostatic Hyperplasia
PSA = Prostate-Specific AntigenWBC, RBC, CBC: (White, Red, Complete) Blood Count
Note • Never do PSA in acute settings PSA = Prostate-Specific Antigen
Diagnosis, Continued • Clinically Andy has acute urinary retention with UTI. He must have residual urine checked by ultrasound or catheterization • Assessment of Andy’s renal function is determined by his age, weight and gender • His renal function is used to determine the acceptable dose for Ciprofloxacin • Andy’s Creatinine Clearance is 75 mL/min which is indicative of very mild renal failure UTI = Urinary Tract Infection
Treatment BID = Bis In Die (Twice Daily)
Discussion • Based on Andy’s history of severe BPH and his acute symptoms, acute urinary retention with urinary tract infection is suspected • He also has very mild renal failure • He needs an indwelling foley catheter and broad spectrum antibiotics while awaiting blood and urine results • A teleconference with the urologist is recommended • Andy needs to be watched very closely; he is in danger of extreme complications because he has untreated retention associated with renal failure • Andy should at least phone you the next day and confirm that he is feeling better. Even if he was feeling better, he might deteriorate again! BPH = Benign Prostatic Hyperplasia
Discussion & Follow-up • Because Andy’s treatment options have been optimized and the BPH progression is still having a profoundly negative effect on his quality of life, Andy is referred to his urologist for urgent consultation • Because he had such long standing severe obstructive and irritative voiding symptoms while on α1-blocker therapy, it is likely that he has chronic retention secondary to BPH and would likely fail a trial of voiding without a catheter. A catheter should remain in place until seen by a urologist. BPH = Benign Prostatic Hyperplasia
Options Pursued by Specialist • Treatment of UTI / prostatitis and AUR as ordered • Initiate treatment again with α1-blockers for short term and 5α-reductase inhibitor for long term • Trial voiding without catheter. If this fails consider cystoscopy and TURP. UTI = Urinary Tract InfectionAUR = Acute Urinary RetentionTURP = Transurethral Resection of the Prostate
At What Point will this Patient Return to his FP and What Should the Specialist Recommend to the FP in Terms of Long Term Follow up?
Family Physician Follow-up • FP can follow up after successful management of AUR (whether trial of voiding was successful or TURP was required) and can follow symptoms, DRE and PSA as per usual. AUR = Acute Urinary RetentionTURP = Transurethral Resection of the ProstateDRE = Digital Rectal ExaminationPSA = Prostate-Specific Antigen