Download
1 / 36
400 likes | 1.22k Vues
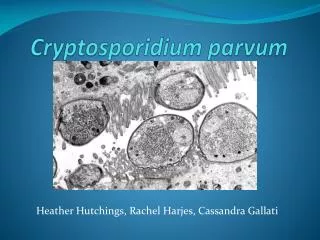
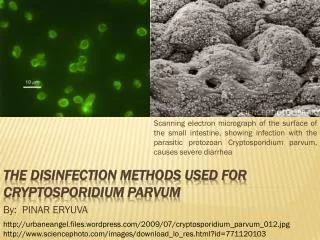
Cryptosporidium parvum. Small in size 5x4.5 μm C. Parvum oocyst. Cryptosporidium parvum. Enteric parasite One of the three most common diarrhea-causing pathogens in the world. Prevalence. Found in most parts of the world Most prevalent in Asia, Africa, Australia, South America

E N D
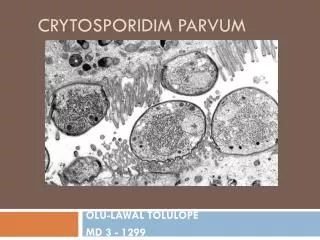
Cryptosporidium parvum Small in size 5x4.5 μm C. Parvum oocyst
Cryptosporidium parvum Enteric parasite One of the three most common diarrhea-causing pathogens in the world
Prevalence • Found in most parts of the world • Most prevalent in Asia, Africa, Australia, South America • Antibody prevalence in Peru and Venezuela – 64% • 32% in Peace Corps workers • More prevalent in rural areas of U.S.
Transmission • Fecal-oral route • Fomites • Water • Drinking water (even after treatment) • Swimming pools • Unpasteurized Apple Cider • Animal contact • Food
Infectivity • Can be infected by just one oocyst • 10 billion oocysts per gram infected feces
Life Cycle Life cycle
Oocyst • Double walled • Resistant to chlorine, drying, progressive freezing, salt water • Only stage in life cycle that can live ex vivo • Imbeds itself in gut epithelium and releases sporozoites • Reproduction continues sexually and asexually
Clinical Characteristics Secretory diarrhea (some mucous, but no blood) Slight fever, fatigue, myalgia Oocysts may infect the lungs and trachea, resulting in cough Dehydration and extreme weight loss in immunocompromised
Laboratory diagnosis of cryptosporidiosis Cryptosporidium spp. • Basic guidelines • A. Multiple stool specimens (at least 3) should be tested before a negative result is reported. • B. To maximize recovery of oocysts, stool specimens in formalin, or other fixatives, should be concentrated prior to microscopic examination (e.g.,10 min at 500 × g when using the formalin
ethyl-acetate concentration procedure). Exception: Specimens to be used for rapid car-tridge assays should NOT be concentrated because antigens are lost during the procedure! • C. Choice of diagnostic techniques depends on available equipment and reagents, experience, • and considerations of time and cost.
1. Wet mount • In bright-field microscopy using differential interference contrast (DIC), oocysts appear as small round structures (4 to 6 μm) similar to yeasts. They do not auto fluoresce.
2. Modified acid-fast stain • Oocysts (4 to 6 μm) often have distinct oocyst walls and stain from light pink to bright red. However, staining may be variable. In particular, infections that are resolving can have colorless oocyst “ghosts.” Mature oocysts may have discernible sporozoites (up to 4). Modified acid-fast oocyst stain
3. Direct fluorescent antibody (DFA) assay • This technique offers the highest combination of sensitivity and specificity and is considered the gold standard by many laboratories. However, it does not provide a stained slide that can be archived. It requires special equipment (fluorescence microscope) and commercially available test kits.
Sensitivity and specificity • Sensitivity and specificityare statistical measures of the performance of abinary classificationtest. Thesensitivity (also calledrecall ratein some fields) measures the proportion of actual positives which are correctly identified as such (i.e. the percentage of sick people who are identified as having the condition); and thespecificitymeasures the proportion of negatives which are correctly identified (i.e. the percentage of well people who are identified as not having the condition.
Definitions Imagine a scenario where people are tested for a disease. The test outcome can be positive (sick) or negative (healthy), while the actual health status of the persons may be different. In that setting: -True positive: Sick people correctly diagnosed as sick -False positive: Healthy people wrongly identified as sick -True negative: Healthy people correctly identified as healthy -False negative: Sick people wrongly identified as healthy
Other methods for detecting Cryptosporidium in stool. 6. Enzyme immunoassay (EIA) The EIA does not rely on microscopy skills, is highly sensitive and specific, and is useful for screening large numbers of specimens.
Cell-free culture ofCryptosporidium parvum • Simple technique for culturing Cryptosporidium without host cell interference. • The potential of improving routine water and other environmental monitoring for Cryptosporidium. • Contribute much to our understanding of the developmental and evolutionary biology of Cryptosporidium.
Amplification of oocysts • In Vivo • - Large animal: Lambs • - Small animal: Neonatal mice • In Vitro • - Cell cuture
In Vitro Cultivation • Oocysts preparation • - neonatal mice • - Inoculation with 100,000-120,000 oocysts per mouse by gastic tube • After 7 day post infection, mice will be • killed and collected intestinal part. • Extraction and purification
In Vitro Cultivation • Media preparation • Excystation media • Sterile Acidic water (pH2.5-3.0) Trypsin EDTA(0.5%) 45 μl
Cell free cultivation • Put 350,000 oocysts from stock into 9 ml of excystation media. • Incubate 30 min at 37 C with shaking every 5 min. • spin down at 3,500 rpm 10 min • Aspirate excystation media • Resuspend pellet with 10 ml of maintenance media and mix well • Add 10 ml of maintenance media into 25cm2 flask • Add 5 ml of oocysts in maintenance media into the flask • Leaving amount of Cryptosporidium oocysts+ maintenance • for checking excystation rate • Incubate at 37 C with 5% CO2
24 hrs after culture trophozoite empty shell Sporozoite
48-72 hrs after culture Meront type 1
48-72 hrs after culture Meront type II
6 day after culture Macrogamete and Microgamete
7-8 after culture • Fertilization and Zygote
After 21 day culture Sporulated oocysts
Treatment • Nitazoxanide • Prevents parasite replication • Immunocompetent • C. parvum will usually pass on its own • Immunocompromised • AIDS patients: treat with antiretrovirals and strengthen immune system, no cure
Prevention • Water filtration • Filters must be <1 um to filter oocyst • Swimming pools • Must be drained if infected fecal accident • Pasteurization • Hand washing • Particularly in daycares
Bottled Waters“not all are created equal” • Water so labeled has been processed by method effective against crypto • Reverse osmosis treated • Distilled • Micro-filtered • Chlorinated • Ozone-treated • Ultraviolet light-treated
Outbreaks • New York 1996; unpasteurized apple cider
Summary Cryptosporidiosis caused by cryptosporidium parvum Transmitted via fecal-oral route Oocyst stage in life cycle is resilient Oocyst imbeds itself in gut epithelium Infection usually occurs from tainted water, even if it has been treated No cure in immunocompromised
My home work Look deeply about : PCR , PROCESSURE AND TYPES