Download
1 / 7
120 likes | 849 Vues
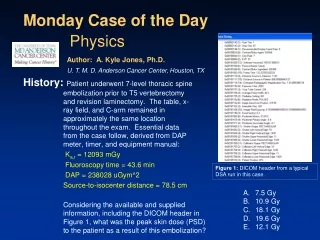
Case of the Day. The likely cause of the poor image quality is: Incorrect collimators used Energy window incorrectly set over scatter below the 140 keV gamma emission photopeak of Tc-99m Scan acquired too soon after injection I-131 NaI in the patient Poor radiolabeling of Tc-99m to the MDP.

E N D
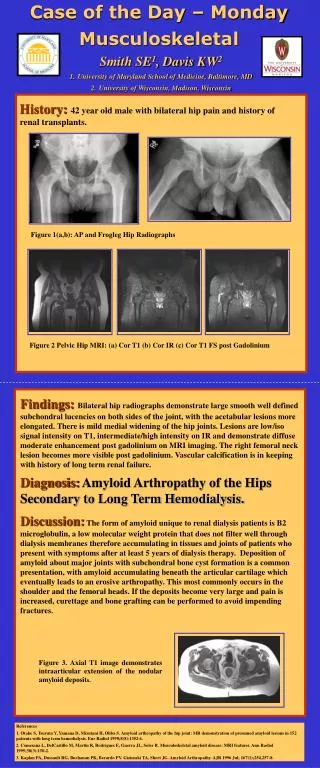
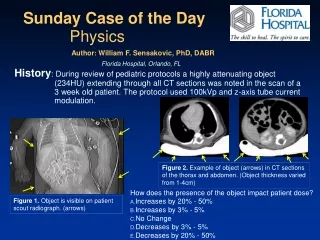
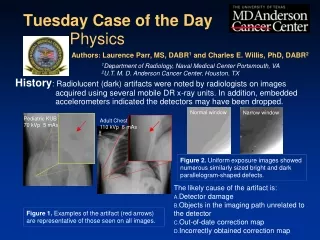
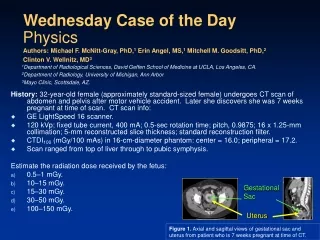
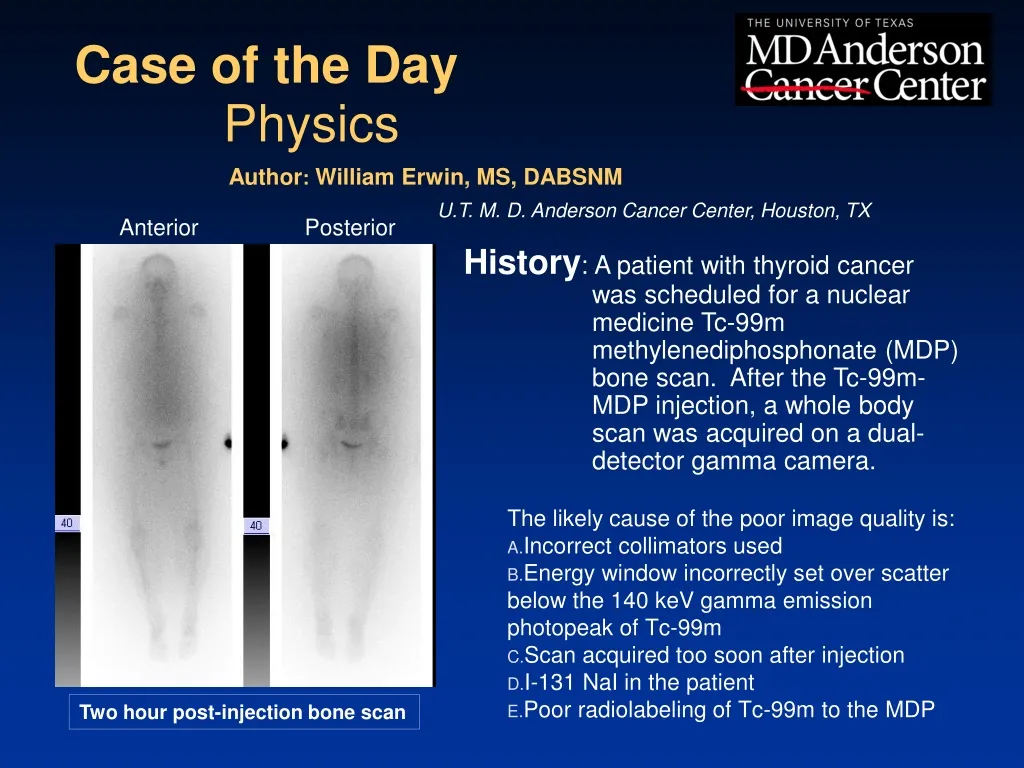
Case of the Day • The likely cause of the poor image quality is: • Incorrect collimators used • Energy window incorrectly set over scatter below the 140 keV gamma emission photopeak of Tc-99m • Scan acquired too soon after injection • I-131 NaI in the patient • Poor radiolabeling of Tc-99m to the MDP • Anterior Posterior Physics Author: William Erwin, MS, DABSNM U.T. M. D. Anderson Cancer Center, Houston, TX History: A patient with thyroid cancer was scheduled for a nuclear medicine Tc-99m methylenediphosphonate (MDP) bone scan. After the Tc-99m-MDP injection, a whole body scan was acquired on a dual-detector gamma camera. Two hour post-injection bone scan
Discussion • The patient received the institution’s standard-of-care, nominal 20 mCi of Tc-99m-MDP, to check for skeletal metastases. • Prior to the bone scan that was performed at two hours post-injection, the patient also received an oral dosage of 5 mCiI-131 NaI for a twenty-four hour thyroid tissue uptake and scan, to be performed the next day.
Discussion (continued) The primary gamma emission of I-131 is 364 keV, and I-131 also emits a 637 keV gamma (albeit with a much lower yield). Low-energy collimators optimized for 140 keV are used for imaging Tc-99m. The collimator septa are purposely thin, to adequately reduce septal penetration of 140 keV photons while minimizing their impact on resolution and sensitivity. A consequence of such “on board” I-131 is Compton scatter photons from the patient, as well as, Compton scatter energy deposited from high energy photons that enter the crystal through the collimator holes or the very thin collimator septa, with energies within the Tc-99m photopeak window used (140 keV +/- 7.5%, or 129.5 to 150.5 keV), being detected as Tc-99m 140 keV primaries. As a result, the Tc-99m scan suffers from a substantial degree of contamination from I-131, including apparent activity outside the patient, rendering the scan non-diagnostic.
Discussion (continued) The patient had to be re-scheduled for a second Tc-99m MDP injection and scan after the I-131 had cleared from the body. When a patient is scheduled for multiple nuclear medicine exams, it is important to schedule them such that the possibility of cross-talk between the different radionuclides administered to the patient is eliminated.
Discussion (continued) If incorrect collimators were used, the sensitivity and resolution would be affected, but the images would still appear as a bone scan. If the energy window incorrectly set over scatter below the 140 keV gamma emission photopeak of Tc-99m, the images would appear as a “fuzzy” bone scan. If the scan acquired too soon after injection, the bone-to-soft tissue contrast would be poor, as the MDP would still be in the early stages of accumulation in bone and clearance from blood and soft tissue. Poor radiolabeling of Tc-99m to the MDP would result in accumulation of free Tc-99m pertechnetate in the stomach wall, thyroid and salivary glands, in addition to the kidneys.
References/Bibliography: Cherry, SR, Sorenson, JA, Phelps ME. Physics in Nuclear Medicine, 4th Ed., Elsevier, Philadelphia, PA, 2012. Bushberg, JT, Seibert, JA, Leidholdt, Jr., EM, Boone, JM. The Essential Physics of Medical Imaging, 3rd Ed., Lippincott Williams & Wilkins, Philadelphia, PA, 2012. Sokole, EB. IAEA Quality Control Atlas for Scintillation Camera Systems,International Atomic Energy Agency, Vienna, 2003. (Available in hard copy, CD-ROM and Internet versions, http://www-pub.iaea.org/books/IAEABooks/6337/IAEA-Quality-Control-Atlas-for-Scintillation-Camera-Systems )