Download
1 / 1
10 likes | 136 Vues
rehabilitation. Progressive Brachial Artery Occlusion Secondary to Remote Radiation Therapy. John M. Lavelle, DO 1 ; Kun Yan, MD 2 1. Boston University Medical Center, Rehabilitation Department 2. Boston VA Healthcare, Physical Medicine And Rehabilitation Service.

E N D
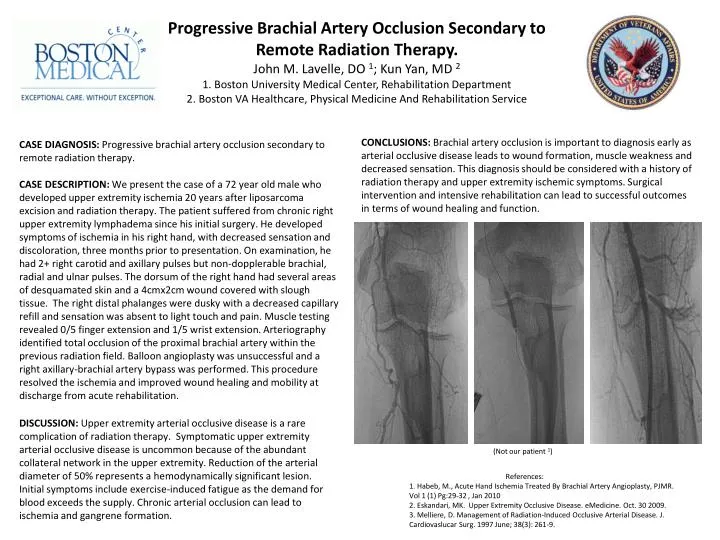
rehabilitation Progressive Brachial Artery Occlusion Secondary to Remote Radiation Therapy. John M. Lavelle, DO 1; Kun Yan, MD 2 1. Boston University Medical Center, Rehabilitation Department 2. Boston VA Healthcare, Physical Medicine And Rehabilitation Service CONCLUSIONS: Brachial artery occlusion is important to diagnosis early as arterial occlusive disease leads to wound formation, muscle weakness and decreased sensation. This diagnosis should be considered with a history of radiation therapy and upper extremity ischemic symptoms. Surgical intervention and intensive rehabilitation can lead to successful outcomes in terms of wound healing and function. CASE DIAGNOSIS: Progressive brachial artery occlusion secondary to remote radiation therapy. CASE DESCRIPTION: We present the case of a 72 year old male who developed upper extremity ischemia 20 years after liposarcoma excision and radiation therapy. The patient suffered from chronic right upper extremity lymphadema since his initial surgery. He developed symptoms of ischemia in his right hand, with decreased sensation and discoloration, three months prior to presentation. On examination, he had 2+ right carotid and axillary pulses but non-dopplerable brachial, radial and ulnar pulses. The dorsum of the right hand had several areas of desquamated skin and a 4cmx2cm wound covered with slough tissue. The right distal phalanges were dusky with a decreased capillary refill and sensation was absent to light touch and pain. Muscle testing revealed 0/5 finger extension and 1/5 wrist extension. Arteriography identified total occlusion of the proximal brachial artery within the previous radiation field. Balloon angioplasty was unsuccessful and a right axillary-brachial artery bypass was performed. This procedure resolved the ischemia and improved wound healing and mobility at discharge from acute rehabilitation. DISCUSSION: Upper extremity arterial occlusive disease is a rare complication of radiation therapy. Symptomatic upper extremity arterial occlusive disease is uncommon because of the abundant collateral network in the upper extremity. Reduction of the arterial diameter of 50% represents a hemodynamically significant lesion. Initial symptoms include exercise-induced fatigue as the demand for blood exceeds the supply. Chronic arterial occlusion can lead to ischemia and gangrene formation. (Not our patient 1) References: 1. Habeb, M., Acute Hand Ischemia Treated By Brachial Artery Angioplasty, PJMR. Vol 1 (1) Pg:29-32 , Jan 2010 2. Eskandari, MK. Upper Extremity Occlusive Disease. eMedicine. Oct. 30 2009. 3. Melliere, D. Management of Radiation-Induced Occlusive Arterial Disease. J. Cardiovaslucar Surg. 1997 June; 38(3): 261-9.