Download
1 / 18
180 likes | 189 Vues
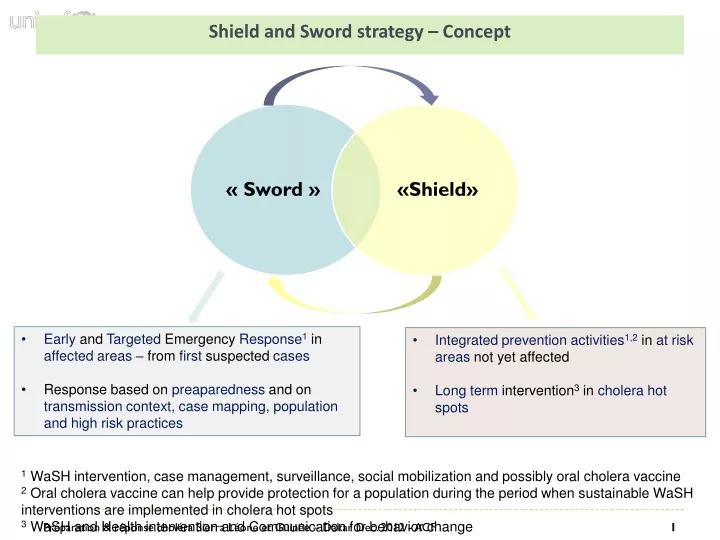
Shield and Sword strategy – Concept. « Sword ». «Shield». Early and Targeted Emergency Response 1 in affected areas – from first suspected cases Response based on preaparedness and on transmission context, case mapping, population and high risk practices.

E N D
Shield and Sword strategy – Concept « Sword » «Shield» • Early and Targeted Emergency Response1in affected areas – from first suspected cases • Response based on preaparedness and on transmission context, case mapping, population and high risk practices • Integrated prevention activities1,2in at risk areas not yet affected • Long term intervention3 in cholera hot spots 1 WaSH intervention, case management, surveillance, social mobilization and possibly oral cholera vaccine 2 Oral cholera vaccine can help provide protection for a population during the period when sustainable WaSH interventions are implemented in cholera hot spots 3 WaSH and Health intervention and Communication for behavior change
Shield and swordstrategy – Directions • Strategy developed by Regional Cholera platform (WCA) following the pilot projects implemented in DRC (2006) and Guinea (2009) • Adjust the WASH responseaccording to transmission context, affected population and case mapping (sword) • Mobility and timeliness of the response (shield and sword) • Protection of population not yetaffected but at risk (shield) Implementing Countries : DRC, Guinea, Guinea Bissau, Niger, Tchad
Emergency response (Sword) – Transmission Context • Adjust the reponseaccording to transmission context Transmission context Targetedresponse Case Investigation
“Compliance with hygiene requirements and traditions • ” • - Procedure supervised by health, religious and traditional authorities • - Limited Number of family members involved (max. 3) • Washing and burial of the body by a trained health worker with a solution containing 2% of HTH • - Burial of the body in the nearest graveyard of the religious group to which the deceased person belong - Disinfect people (hand and cloths) in charge of washing and burying the body Washing and burial of the body Excreta and vomit on the body Propose three alternatives to the family of the deceased: 1 – Incinerating the clothes 2 – Burying the deceased with their clothes 3 – Soaking them for 2h in a 0.2% HTH solution and cleaning with soap Clothes of the dead Equipment used for washing and burial 2% HTH disinfection carried out by a trained health worker Massive spraying with a solution containing 2% HTH and collection of excrements on the floor carried out by trained health worker Excreta and vomit on the floor
Option 1: If the ban on ceremonies is an obstacle to the management of deaths, the ceremony should be accompagned by Health promoters • Hand Washing Station • Distribution of hygiene kits : soap and products to disinfect water • Key messages on hand Washing at key moment Funeral, moorningceremony Greetings Water Common meals Kettles and cups Nats Option 2: Health authorities mobilize administrative, traditional and religious authorities per community in order to prohibit / postpone mortuary places/funerals following cholera-related deaths
Prepare chlorinated solutions 0,02%, 0,2%, 2% • Disinfect faeces and vomit of patients: Put in the bucket 2cm of 2% solution. Dispose in a safe place • Clean the facility two to three times a day: disinfect beds, floors, latrines, empty the rubbish… • Inform caretakers about the different kinds of solutions: drinking water, ORS, dishes/clothes… • Controlingall entries and exists • No visitorsallowed • Maximum 1 caretaker per patient • Disinfectfeet, hands, dishes, clothes, etc. • Disinfect transportation means(0,2%) and attendant/drivers Cholera Treatment Facilities Sharing food & dishes Contaminated food and water Patients Buckets Washing clothes Care Taker Sensitize all caretakers on how cholera is transmitted and how they can protect themselves from cholera – Give 1 NFI kit to the caretaker after admission Visit to the sickperson Greetings Food, cloth & utensils water and contaminated food Hand / vehicules Attendant Location of the tratmentfacilities • Disinfect dead bodies following carefully the guidelines and procedure • Disinfect water points neraby the health centre frequently Borehole, wells, gamess Health and Hygiene staff • Disinfect all items of patients and caretakers before their discharge (dishes, clothes,etc) with 0,2% • Inform caretakers and patients of possible transmission of cholera even after discharge. Chlothe, material, handss
“Household visits” • IEC and distribution of hygiene kits in all the households of the compound affected • Soaking patient’s clothes and bedding for 2 hours with an 0.2% HTH solution • Washing the dishes, kettles and cleaning ustensilswith an 0.2% HTH solution • Disinfection of excreta with a 2% HTH solution and cleaning up with DOL • Chlorination of water storage containers with an appropriate disinfectant • Washing of the water drawing bucket with a 0.2% HTH solution • Active case finding by the authorities for early referral Household transmission Cloth and bedding, dishes, kettles, cleaning, water,meals, excreta, etc Contamination in affected compound • Raising awareness about the risk of contamination of neighbors and family members during visits of the patient at home before admission and after discharge (after assessing risks of stigma and impacts). • Raising the awareness of religious and traditional authorities during sermons using town criers about the risks associated with household visits (after assessing risks of stigma and impacts). • Prior to their discharge medical staffs raising patients and caretakers’ awareness on the possible cholera transmission once going back to their home Contamination followingvisits Greeting Water Common meals
Gatherings • Hand Washing Station • Distribution of hygiene kits : soap and products to disinfect water • Key messages on hand Washing at key moment Ceremony • Hand Washing Station • Distribution of hygiene kits : soap and products to disinfect water • Key messages on food preparation Street restaurant Public places (markets, etc) Greeting Water Meals Greeting Water Meals Greeting Water Meals Greeting Water Meals • - Sketches, hand-washing games and movies • Hand-washing Station • Distribution of hygiene kits in schools • Control of food sold in schools • Closing of schools during cholera outbreaks School • - Mass sentization • Hand-washing Station
Nomadism Social and livelyhood group Talibe Seasonal and collective fishing Gold miners
Water point desinfection • Household chlorination • IEC and water disinfectant distribution • Develop a water disinfectant supply chain and social marketing programme (Sûr'Eau, Lifeguard) • Promote the use of natural water disinfectants (Moringa) • Disinfection at source • Buckets chlorination (shortage, poor community acceptance of household chlorination) • Mobilization of administrative and traditional authorities • Prohibit the consumption of surface water for domestic and recreational use Surface water • Household chlorination (private and not improved well) • Bucket chlorination (share well) • Well chlorination (imporved facilities and dayly follow up) Open well Hand pump Defecation Run off Washing patient’s clothes, Children’s games Run off Dirty Hand during transport and conservation Run off Pipes leakages - Chlorination, maintaining between 0.5 and 1 mg/l FRC at network exit; Water network • Household chlorination • Bucket chlorination (share hand pump)
Control washing and burial of the body Emergency Response – Response mechanism in rural areas In CTC / UTC by healthworkers Check by communityhealthworkers Earlydetection and referral Case investigation Transmission associatedwithfuneral rites Investigation Form Mobilization of local and traditional leaders Control of funerals
Emergency Response – Response mechanism in urban areas In CTC / UTC or duringhouseholddesinfection Healthworkers and WASH actors Case Mapping Field investigation in permanent cluster Transmission to workers in Harbour Transmission to childrenthroughgames Water-borne transmission: Water vendor Pipes leakages Training water vendorchlorination Water pipes repaired by NSWS Focus group and hygiene kit distribution IEC throughgames and movie
Emergency Response – Protection of population not yet affected Anticipate where cholera is going to spread Get ready when cholera is nearby Spreading point Increase surveillance Increase FRC In water network Population mouvement Inform and train community leaders ahead Population gathering Pre-positioning of Wash and Health items
Emergency Response – Indicators monitoring • Household transmission Householdvisits • Improvedknowlegde of broadcast messages (75 % of messages are integrated by households – Monthly trend) • % of home visited and delay of intervention • 0 contamination followingvisits to the sickperson at home • Transmission in linkwith CTC/CTU Case isolation • 0 contamination in linkwith CTC/CTU once case isolation is put in place • Water-borne transmission • Water network cholrination: 0,5 to 1mg/l of FRC in water network • Householdchlorination: 75% of households have FRC in drinking water at home (entre 0,5 et 1mg/l)
Emergency Response – Indicators monitoring • Transmission in linkwithlivelyhoodgroups – Ex street restaurant • Free ResidualChlorine in drinking water (between0,5 and 1mg/l), hand washing station with soap • % of community workers/leaders that are informed about population movements and assemblies before they take place (weddings, festivals, funerals, nomadism, etc.). • Population and leaders recognize the disease • % of head of households who can describe the symptoms (strong liquid diarrhea with or without vomiting) ; • % of heads of household who know that rapid rehydration is vital to ensure survival; • % of persons who go quickly to health centers within the first 24h; • % of community workers/leaders that are informed about suspected cholera cases quickly, within 24h; • % of schools that pass on key messages to children (symptoms, referal, prevention);
Emergency Response – Indicators strategic • WASH & Epidemiology targeting is working • % of WASH interventions in communities that are based on transmission context identification (geographical origin, types of communities, high-risk practices); • Impact of the response • Decrease of weeklyattack rate in intervention areas (drop after 3 weeks) • Effectiveness of the response • Delay between first case registration and response