Download

1 / 39
551 likes | 2.59k Vues
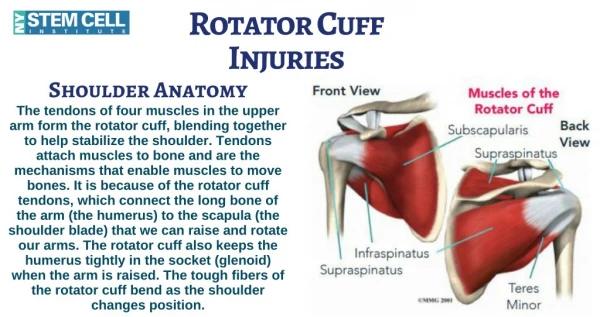
IRREPARABLE ROTATOR CUFF TEAR . NADHAPORN SAENGPETCH. DEFINITION. Massive rotator cuff tears that are not reparable by conventional means. Their size and retraction, cannot be repaired to their insertion on the tuberosities despite conventional techniques.

E N D
IRREPARABLEROTATOR CUFF TEAR NADHAPORN SAENGPETCH
DEFINITION • Massive rotator cuff tears that are not reparable by conventional means. • Their size and retraction, cannot be repaired to their insertion on the tuberosities despite conventional techniques. • associates with a high-riding humeral head
FACTS • unknown true incidence • may have no symtoms/mild/severe pain • associated with concomitant glenohumeral OA • asymtomatic tears in elderly found 30-50% Zlatkin MB. J Bone Joint Surg Am.1995; 77:10-5. • age > 70 ; found FTRCT 38% Tempelhof et al. J Shoulder Elbow Surg. 1999;8:296-9.
57 patients Infraspinatus degeneration had a highly negative influence on the outcome of supraspinatus repairs. It worsens with time. The subscapularis rarely degenerate, even when its tendon is not torn. Goutallier D.Clin Orthop Relat Res. 1994 Jul;(304):78-83. Cuff Atrophy & Fatty Infiltration
Goutallier Classification : 5 stages 0 : no fat 1: minimal fat 2 : muscle>fat 3 : muscle=fat 4 : muscle<fat
2 PHYSIOLOGICALLY DISTINCT GROUPS OF PATIENT • Older > 70, lower-demand who have been asymtomatic until minor trauma created symtoms • Younger, more active with dramatic symtoms of pain and disability after an acute event / with a history of cuff injury
2 DISTINCT ANATOMIC PATTERNS • Posterosuperior failure* : supraspinatus, infraspinatus and teres minor tendons • Anterosuperior failure : supraspinatus and subscapularis tendons ± LHB ۩Loss of the coracoaromial arch and anterosuperior instability humeral head migration
PATHOMECHANICS • The RC acts as a dynamic stabilizer, resisting upward motion of a humeral head during deltoid contraction. • Irreparable cuff : loss a force couple, allow a humeral head migrates superiorly during deltoid contracts (superior shoulder instability)
CLINICAL PRESENTATIONS • pain • deficit ROM • atrophy of scapular muscles • crepitus and hemarthrosis • Posterosuperior disruption : AB, FE and active ER • Anterosuperior disruption : AB, IR
Posterosuperior Disruption External rotation lag sign
Posterosuperior Disruption Hornblower’s sign*
Anterosuperior Disruption Belly press test
Anterosuperior Disruption Lift-off sign
RADIOGRAPHIC FINDINGS • Position of the humeral head • Evidence of glenohumeral OA • Disorder of the AC joint
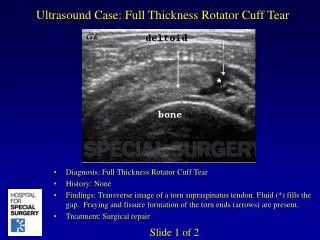
MRI VS MR Arthrography • 41 shoulders had MRI followed by MR arthrography • Sensitivities for detecting full-thickness rotator cuff tears by MRI and MR arthrography were 90.2 and 100% respectively. • more accurate in evaluating rotator cuff tear size and morphologic features • morphologic classification of the torn tendon: blunt end, tapering end, indistinct end, horizontal tear, and global tear Toyoda H. Clin Orthop Relat Res. 2005 Oct;439:109-15.
MANAGEMENT • depends on the presenting symtoms, age and functional level • medical comorbidities, an intact coracoacromial arch and concomitant arthritis • no evidence-based, prospective, matched- patient studies comparing nonsurgical and surgical treatments
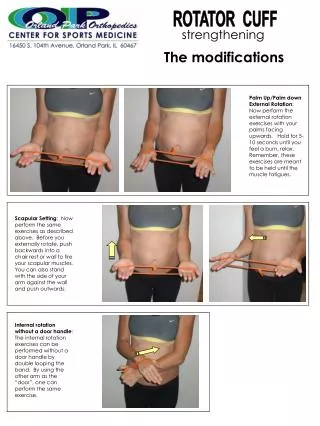
NONOPERATIVE TREATMENT • relieve pain & create biomechanically compensated function by muscle substitution • NSAIDs • steroid injection • local therapeutic modalities • strengthening exercise • > 3 months to succeed
SURGICAL TREATMENTS • Subacromial débridement, partial repair, cuff débridement and biceps tenotomy • Reconstructive procedures • Conventional and reverse arthroplasty • Glenohumeral arthrodesis
SUBACROMIAL DÉBRIDEMENT • Healthy, low-demand with pain • A patient with positive for impingement test is a good surgical candidate. • Procedures : limited, acromial smoothening, bursectomy No release of the CA ligament
PARTIAL REPAIR • “Suspension bridge model” restore continuity between anterior and posterior portions of the tear resulted in a fibrous frame close to the equator of the head. • Create a force to stabilize the head against the glenoid and enabling full function of deltoid Burkhart S. Arthroscopy . 1994;10:363-70.
CUFF DÉBRIDEMENT • Rockwood : open acromioplasty, decompression, cuff débridement • Ellman : pain relief, but no significant increase in strength and ROM • Zvijac and Kempf : substantial deterioration in pain relief/strength/functional outcome
TENOTOMY OF LHB • Anterosuperior lesion • No effect on the ROM or strength Walch G. J Shoulder Elbow Surg. 2005:14: 238-46.
TUBEROPLASTY • Open surgery • Shaving and reshaping of the overhanging bone at GT to create a recontoured subacromial space Fenlin JM Jr. J Shoulder Elbow Surg. 2002;11:136-42.
TENDON TRANSFERS • Transfer : the existing cuff tendons, other periscapular muscles, grafts or synthetic substitution • Young, good deltoid function • Posterosuperior : latissimus dorsi • Anterosuperior : pectoralis major (sternal head)
TENDON TRANSFERS Pectoralis major Latissimus dorsi
TENDON TRANSFERS • Gerber : good-to-excellent results > 10 yrs, better result with intact subscapularis • Iannotti : EMG study in latissimus dorsi transferred patients; had activity with adduction but no activity with active FE/ER • Concept of a tenodesis effect
TENDON TRANSFERS • Latissimus dorsi : clinical results sex (male), preoperative shoulder function and general strength (Iannotti JP. J Bone Joint Surg Am. 2006;88:342-348) • Pectoralis major : if the SS tear associated with irreparable Sup. tear, tendon transfer may not be warranted. (Jost B.J Bone Joint Surg Am.2003;85:1944-1951)
TENDON TRANSFERS • Complex, need a long period of rehab, limited • Not indicated for older, more debilitated patients • Synthetic allograft patches : can create foreign body reactions leading to rejection & cannot replace RC functions
ARTHROPLASTY • Concomitant with arthritis or instability • Conventional VS Reverse ball and socket prosthesis
CONVENTIONAL ARTHROPLASY • HEMIARTHROPLASTY • Indications : intact coracoacromial arch good deltoid function no previous acromioplasty no anterosuperior instability • Contraindication : pseudoparalysis of shoulder
REVERSE ARTHROPLASTY • RC tear + arthritis + pseudoparalysis • Unknown long-term results • Medialize the centre of rotation • Increasing the deltoid lever arm • Glenoid loosening (notching), hematoma and instability
GLENOHUMERAL ARTHRODESIS • Deltoid and RC are not function. • High-demand, require a strong stable shoulder girdle • Limited rotation • nonunion