Download
1 / 1
10 likes | 145 Vues
The Effect of Tumor Bed Location on Heart Dosimetry for 3-D Conformal Partial Breast Irradiation and Comparison with Whole Breast Irradiation. Ashley Gale, M.S., Anudh Jain, M.D. Laura Vallow, M.D. Department of Radiation Oncology Mayo Clinic, Jacksonville, Florida. BACKGROUND

E N D
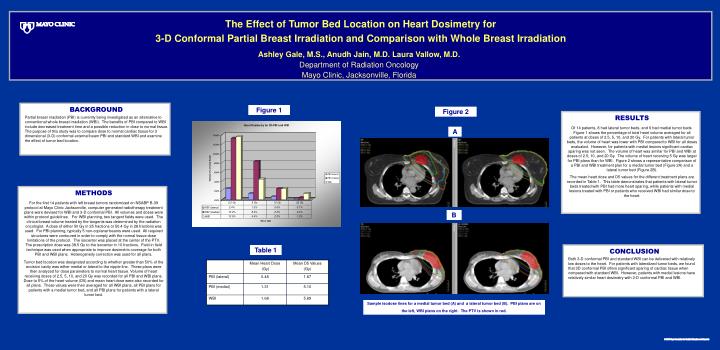
The Effect of Tumor Bed Location on Heart Dosimetry for 3-D Conformal Partial Breast Irradiation and Comparison with Whole Breast Irradiation Ashley Gale, M.S., Anudh Jain, M.D. Laura Vallow, M.D. Department of Radiation Oncology Mayo Clinic, Jacksonville, Florida BACKGROUND Partial breast irradiation (PBI) is currently being investigated as an alternative to conventional whole breast irradiation (WBI). The benefits of PBI compared to WBI include decreased treatment time and a possible reduction in dose to normal tissue. The purpose of this study was to compare dose to normal cardiac tissue for 3 dimensional (3-D) conformal external beam PBI and standard WBI and examine the effect of tumor bed location. Figure 1 Figure 2 RESULTS Of 14 patients, 8 had lateral tumor beds, and 6 had medial tumor beds. Figure 1 shows the percentage of total heart volume averaged for all patients at doses of 2.5, 5, 10, and 20 Gy. For patients with lateral tumor beds, the volume of heart was lower with PBI compared to WBI for all doses evaluated. However, for patients with medial lesions significant cardiac sparing was not seen. The volume of heart was similar for PBI and WBI at doses of 2.5, 10, and 20 Gy. The volume of heart receiving 5 Gy was larger for PBI plans than for WBI. Figure 2 shows a representative comparison of a PBI and WBI treatment plan for a medial tumor bed (Figure 2A) and a lateral tumor bed (Figure 2B). The mean heart dose and D5 values for the different treatment plans are recorded in Table 1. This table demonstrates that patients with lateral tumor beds treated with PBI had more heart sparing, while patients with medial lesions treated with PBI or patients who received WBI had similar dose to the heart. A METHODS For the first 14 patients with left breast tumors randomized on NSABP B-39 protocol at Mayo Clinic Jacksonville, computer generated radiotherapy treatment plans were devised for WBI and 3-D conformal PBI. All volumes and doses were within protocol guidelines. For WBI planning, two tangent fields were used. The clinical breast volume treated by the tangents was determined by the radiation oncologist. A dose of either 50 Gy in 25 fractions or 50.4 Gy in 28 fractions was used. For PBI planning, typically 5 non-coplanar beams were used. All required structures were contoured in order to comply with the normal tissue dose limitations of the protocol. The isocenter was placed at the center of the PTV. The prescription dose was 38.5 Gy to the isocenter in 10 fractions. Field in field technique was used when appropriate to improve dosimetric coverage for both PBI and WBI plans. Heterogeneity correction was used for all plans. Tumor bed location was designated according to whether greater than 50% of the excision cavity was either medial or lateral to the nipple line. These plans were then analyzed for dose parameters to normal heart tissue. Volume of heart receiving doses of 2.5, 5, 10, and 20 Gy was recorded for all PBI and WBI plans. Dose to 5% of the heart volume (D5) and mean heart dose were also recorded for all plans. These values were then averaged for all WBI plans, all PBI plans for patients with a medial tumor bed, and all PBI plans for patients with a lateral tumor bed. B Table 1 CONCLUSION Both 3-D conformal PBI and standard WBI can be delivered with relatively low doses to the heart. For patients with lateralized tumor beds, we found that 3D conformal PBI offers significant sparing of cardiac tissue when compared with standard WBI. However, patients with medial lesions have relatively similar heart dosimetry with 3-D conformal PBI and WBI. Sample isodose lines for a medial tumor bed (A) and a lateral tumor bed (B). PBI plans are on the left, WBI plans on the right. The PTV is shown in red.






















