Download
1 / 84
950 likes | 1.48k Vues
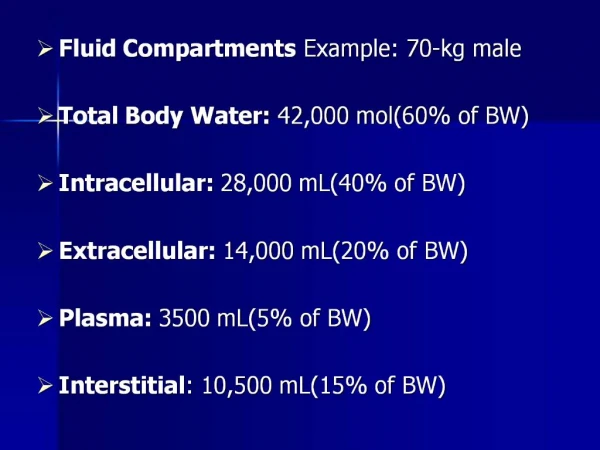
Fluids & Electrolytes. Body water and fluid volumes:. Water constitutes 50% to 70% of lean body weight . Total body water. intracellular fluid compartment (40% of body wt). Extracellular fluid compartment (20% of body wt). plasma 5% of body wt .

E N D
Body water and fluid volumes: • Water constitutes 50% to 70% of lean body weight . • Total body water. • intracellular fluid compartment (40% of body wt). • Extracellular fluid compartment (20% of body wt). plasma 5% of body wt . An interstitial compartment 15% of body wt.
Blood volume of an adult: • Blood volume of an adult is 5 L-7L OF normal body weight or 70 ml/ kg. • Blood volume consists of plasma erythrocyte volumes. 70 kg man has a TBW of 42 L. ECF is 1/3 TBW ( 14 L ). Plasma 1/4 (5%) ECF ( 3.5 L ). Hematocrit of 40% >>> 1.5 L RBC volume >>>> 3.5L + 1.5L = 5L
:Ions and osmolality • K & Mg are the major IC cations. • Na is the major EC cation. • Balance between the EC and IC ions is maintained through the osmolality and active transporter Na/K ATP pump. ( if ATP depleted >>> cellular dysfunction). • Osmolality: is the concentration of solute in the solution (determined by ionic conc. Of the dissolved substances per unit solvent). • The normal blood osmolality is 300 mosm. • Osmolality : 2Na +glucose +BUN =300_+15.
:Ions and osmolality • What is the main regulator of osmolality? • ADH - As osmolality > 300 mosm , osmoreceptor cells in the supra- optic nuclei of the hypothalamus signal the posterior hypothalamus to increase production of ADH. - ADH increases water absorption from distal renal tubules.
Fluid & electrolyte requirements: • The approximate daily fluid requirements for an individual is based on body weight at room temperature : The 1st 10 kg >>> 100 ml/kg/day ~ 4 ml/kg/hr The 2nd 10 kg >>> 50 ml/kg/day ~ 2 ml/kg/hr Wt. above 20kg >>> 20 ml/kg/day ~ 1 ml/kg/hr
Fluid & electrolyte requirements • How much fluid would an average adult (70kg) need in a day? • 2500 ml ( 1000 ml + 500 ml + 1000 ml )>>>>normal saline
Fluid & electrolyte requirements • The approximate daily electrolytes requirement is as follows: Na+, K+, Cl- >>>> 1 mEq/kg/day each Ca++ >>>> 2 g/day Mg++ >>>> 20 mEq/day N.B: neither Ca++ nor Mg++ is necessary in maintenance IV fluid.
Fluid & electrolyte requirements • Sources of insensible fluid loss in a healthy adult are: - Respiratory>> 600ml/day - Skin >> 400ml/day ( In fever, insensible skin loss can increase up to 250 ml/day/degree of fever ). - Stool >> 200 ml/day
Evaluation of intravascular volume: • Intravascular volume can be assessed using history ( heat expoure - vomiting – diarrhea) physical examination or lab. Examinations. 1- Physical examination: ( Signs) • Hypovolemia: • skin turgor • hydration of mucous membranes • palpation of peripheral pulses • resting heart rate • BP and their orthostatic changes • urine output • Hypervolemia: • pitting edema • increased urinary output • signs of pulmonary edema
Evaluation of intravascular volume 2- Lab. Investigations: • Hypovolemia : • rising hematocrit. • metabolic acidosis. • urine specific gravity >1.010. • urine sodium <10 mEq/L. • urine osmolality > 450 mOsm/kg. • hypernatraemia. • BUN / creatinine > 10:1. • Hepervolemia: • radiographic signs of increased pulmonary vascular and interstitial markings “ Kerly B lines” or diffuse alveolar infiltrates).
Evaluation of intravascular volume 3- Hemodynamic measurements: A. CVP ( indicated when volume status is difficult to assess or when rapid or major alterations are expected). • Hypovolemia : CVP < 5 mm Hg, small elevation ( 1- 2 mm in response to 250 ml fluid bolus ). • Hypervolemia : CVP > 12 mm Hg (in the absence of Rt ventricular dys- function, increased intrathoracic pressure, restrictive pericardial). B.Pulmonary artery pressure.
Intravenous Fluids: • IV fluid therapy may consist of infusions of crystalloids, colloids, or a combination of both. • Crystalloids : • Aqueous solutions of LMW salts with or without glucose. • They rapidly equilibrate with and distribute throughout the ECF space. • Colloids : • contain high MW substances such as proteins or large glucose polymer. • They maintain plasma oncotic pressure and remain mainly intravascularly.
Intravenous Fluids • General principles: 1- Crystalloids when given in sufficient amounts can be just as effective as colloids in restoring intravascular volume. 2-Replacing an intravascular volume deficit with crystalloids generally require 4 X the volume needed using colloid
Intravenous Fluids • General principles: 3-Most surgical patients have an ECF deficit that exceeds the ICF deficit. 4- Severe intravascular fluid deficits can be more rapidly corrected using colloid solutions. 5-The rapid administration of large amounts of crystalloids (> 4-5 L ) is more frequently associated with significant tissue edema. ( marked tissue edema can impair oxygen transport, tissue healing and return of bowel Function following major surgery ).
Intravenous Fluids 1- Crystalloid solutions: • Includes a wide variety of solutions. • Intravascular half life is 20 – 30 minutes. • Solutions are chosen according to the type of fluid loss: • Maintenance solutions. ( Hypotonic solutions in cases of primarily water deficit). • Replacement solutions. ( Isotonic solutions in cases of both water and electrolyte deficits). N.B: Glucose is provided in some solutions to maintain tonicity or to prevent ketosis and hypoglycemia due to fasting. ( Children and women more prone to hypogly.).
Intravenous Fluids • Crystalloids • Since most intraoperative fluid losses are isotonic, replacement type solutions are generally used. • The most commonly used fluid is lactated Ringer’s solution: - slightly hypotonic and tends to lower serum Na+ to 130 mEq/L. - Generally it has the least effect on ECF composition, and it is the most physiologic solution when large volumes are needed. - Lactate is converted by the liver into bicarbonate.
Intravenous Fluids • Crystalloids • Normal Saline: - When given in large volumes, it produces dilutional hyperchloremic acidosis bec. Of its high Na+ & Cl- contents ( Plasma bicarbonate conc. decreases as Cl- conc. Increases). - Thus, NS is a preffered solution in for hypochloremic metabolic alkalosis and for diluting PRBCs prior to transfusion.
Intravenous Fluids • Crystalloids • D5W: - Used for replacement of pure water deficits and as a maintenance fluid for patients on sodium restriction. • Hypertonic 3% saline: - Treatment of severe symptomatic hyponatremia. NB: 3% - 7.5% saline solutions are used in resuscitation of patients in hypovolemic shock (they must be administered slowly , preferably through CVP, bec they readily cause hemolysis).
Intravenous Fluids 2- Colloid solutions: • Intravascular half life 3 – 6 hours (because the osmotic activity of its high MW substances tends to maintain it intravascularly). • The substantial cost and occasional complications tend to limit their use. • Generally accepted indications for use: • Severe intravascular fluid deficits ( hemorrhagic shock) prior to arrival of blood for transfusion. • Severe hypoalbuminaemia or conditions associated with large protein losses such as burns.
Intravenous Fluids • Colloids • Several colloid solutions are generally available. • They are derived from either plasma proteins or synthetic glucose polymers, and they are supplied in isotonic electrolyte solutions.
Intravenous Fluids • Colloids • Blood derived colloids: - includes albumin (5% and 25% solutions) and plasma protein fraction (5%). - Both are heated to minimize the risk of hepatitis and other virally transmitted diseases. - Plasma protein fraction is associated with hypotensive reactions ( allergic).
Intravenous Fluids • Colloids • Synthetic colloids: -include dextrose starch and gelatins. ( gelatins are associated with histamin mediated allergic reactions and are not available in the USA). - Dextrose starches include Dextran and Hetastarch. 1-Dextran is available as dextran 70 and Dextran 40. When infused in a rate more than 20ml/kg/d, they will be associated with certain complications.
Intravenous Fluids • Colloids • Complications associated with Dextrans: - Interfering with blood typing. - Prolong bleeding time ( antiplatelets effect). - Renal failure. - Anaphylactic reactions ( mild – severe).
Intravenous Fluids • Colloids 2- Hetastarch is highly effective as a plasma expander and less expensive than albumin. - It is non antigenic ( thus anaphylactic reactions are rare). - Coagulation and bleeding times not significantly affected. • Pentastarch ( LMW starch solution, is less likely to cause adverse effects and may replace hetastarch.
Acute electrolyte imbalance • Disorders of Sodium balance. • Disorders of Potassium balance. • Disorders of Calcium balance. • Disorders of Phosphorus balance. • Disorders of Magnesium balance.
Disorders of Sodium balance Physiology : • The normal individual consumes 3-5g/day NaCl. • Balance is maintained primarily by the kidneys. • Normal Na concentration is 135-145 mmol/l . • Potential sources of significant Na loss included sweat ,urine and gastrointestinal secretions. N.B. Na concentration and total body water are controlled by independent mechanism, As a consequence hypo and hypernatremia may occur in conjugation with hypovolemia, hypervolemia or euvolemia, thus it is necessary to measure the osmolality to evaluate the patient with hyponatremia. • Na concentration largely determines the plasma osmolality (Posm) which can be approximated by the following equation.
Disorders of Sodium balance • Na concentration largely determines the plasma osmolality (Posm) which can be approximated by the following equation :
hyponatremia • Hyponatremia : • Low serum [Na] <135. • Due to :- Loss of Na . - Gain of H2O. • Main regulation of the Na extracellular osmolality ---hypothalamus • Nausea + ADH low Na /K • Cause of ADH : - hypernatremia - hypovolemia - brain occupied lesion - truma - drug :acting centrally morphine –pethidine – NASID - Li+ - pain - nausea , vomiting - SIADH: low plasma osmolality (<280 mOsm/L),Hyponatremia (<135mmol/L),low urine output with concentrated urine (>100 mOsm/kg),elevated urine sodium (>20mEq/l), clinical euvolemia
Disorders of Sodium balance Hyponatremia : Causes and diagnosis : Hyponatremia may occur in conjunction with hyper tonicity ,isotonicity or hypo tonicity so it is necessary to measure the serum osmolility to evaluated patients with hyponatremia. • Isotonic hyponatremia : OSMOLILITY :280-290 mOsm Note : measure blood glucose ,lipid , protein • Pseudohyponatremia : • Hyperlipidemia • Hyperproteinemia • Isotonic infusions : • Glucose • Mannitol • Glycine • TURP:
Disorders of balance Sodium 2- Hypertonic hyponatremia (>290 mOsm ): Note : measure blood glucose . • Causes : • Hyperglycemia : • Hypertonic infusions: • Glucose • Mannitol • glycine • TURP: • hyponatremia in conjunction with cardiovascular and neurological manifestation , which infrequently follow transurethral resection of prostate Results from intraoperative absorption of significance amounts of irrigation of fluid (glycerine, sorbitol, mannitol) may occur in isotonic ,hypotonic , hypertonic hyponatremia
Disorders of Sodium balance 3- hypotonic hyonatremia: (<280 mOsm) Is classified on basis of extracellular fluid volume Generally developed as a consequence of the administration and retention of hypotonic fluids [ dextrose 5% in water ,0.45% Nacl . 1. Hypovolemic hypotonic hyponatremia : In the surgical patient most commonly results from replacement of sodium –rich fluid losses (from the GI tract, skin or lungs)with an insufficient volume of hypotonic fluid . • GI losses • Skin losses • Lung losses • Third –space losses • Renal losses
Disorders of Sodium balance 2.Hypervolemic hypotonic hyponatremia : The edematous states of congestive heart failure , liver disease , nephrosis occur in conjunction with inadequate circulating blood volume renal retention renal retention of sodium and water disproportionate accumulation of water hyponatremia
Disorders of balance Sodium 3. Isovolemic hypotonic hyponatremia : • Water intoxication • K losses • Reset osmostat • SIADH: low plasma osmolality (<280 mOsm/L),Hyponatremia (<135mmol/L),low urine output with concentrated urine (>100 mOsm/kg),elevated urine sodium (>20mEq/l), clinical euvolemia • Drugs: sulfonylureas – carbamazepine – phenothiazines -antidepressnts
Disorders of Sodium balance • Clinical manifestation : • Symptoms associated with hyponatremia are predominantly neurological . • Posm intracellular water influx intracellular volume cerebral edema • Mild to moderate hyponatremia ( Na+ > 125 mEq/L ) Asymptomatic. • Early symptoms: >>> Non specific anorexia, nausea, weakness. • Severe hyponatremia ( Na+ < 120 mEq/L) >>> lethargy, confusion, seizures, coma, death.
Disorders of Sodium balance treatment • Isotonic and hypertonic hyponatremia : Correct with resolution of under lying disorder. • Hypovolmic hyponatremia : administration of 0.9% NaCL to correct volume deficits and replace ongoing losses . • Water intoxication :fluid restriction (1000ml/day) • SIADH: water restriction (1000ml/day)initially ,then a loop diuretic (furosemide ) or an osmotic diuretic (mannitol ).
Disorders of Sodium balancetreatment • Hypervolmic hyponatremia : • Water restriction to return Na to greater than 130 mmol /L. • Optimizing cardiac performance in case of severe congestive heart failure. • If the edematous hyponatremic patient becomes symptomatic plasma NA can be Increased to safe level by the use of a loop diuretic ( furosemide ,20-200mg IV every 6 hr )and replacing urinary Na losses with 3% Nacl ,reasonable approach is to replace approximately 25%of the hourly urine output with Nacl ,hypertonic saline should not be administration to these patients without Concomitant diuretic therapy. • Administration of synthetic brain natriuretic peptide (BNP) is also therapeutically in the setting of the acute heart failure because it inhibit Na reabsorption at the cortical collecting duct failure because it inhibits the action of vasopressin on water permeability at the inner medullary collecting duct.
Disorders of Sodium balance treatment In the presence of symptoms or extreme hyponatremia [Na<110mmol/L]: Hypertonic saline (3%Nacl )is indicated to correct serum Na to 120mmol/L. The quantity of 3% Nacl that is required to increase serum Na to 120mmol/L can be estimated by calculating the Na deficit: Na deficit (mmol)=0.6xlean body weight (kg)x[120-measured serum Na (mmol/L)] . Central pontine demylination occurs in the setting of correction of hyponatremia , the risk factors for demyelination are contraversial but appear to be related to chronicity of hyponatremia (>48hr) and the rate of correction .
Disorders of Sodium balance hypernatremia • Hypernatremia: • Is uniformal hypertonic and typically the result of water loss in excess of solute . • Patients are categorized on the basis of their extracellular fluid volume status
Disorders of Sodium balance hypernatremia • Clinical manifestation : Symptoms are primarily neurologic • Lethargy. • Weakness. • Irritability . • Fasciculations . • Seizures. • Coma. • Irreversible neurologic damage .
Disorders of Sodium balance hypernatremia Diagnostic approach to hypernatremia : Clinically assess ECF volume • Depleted :hypovolemic hypernatremia :loss of water and sodium • Renal (diuretics – glycosuria – urea diuresis – acute and chronic renal failure –partial obstruction ) • GI losses (diarrhea) • Respiratory losses • Skin losses (burns) • Adrenal insufficiency
Disorders of Sodium balance hypernatremia 2. ECV normal : isovolemic hypernatremia :loss of water: • Diabetes insipidus : • Characterized by polyuria and polydipsia in association with hypotonic urine (urine osmolality <200 mOsm/kg ) and high plasma osmolality (>287mOsm/kg ) • Types of DI : • central diabetes insipidus(CDI) : - a defect in the hypothalamic secretion of ADH . - head trauma , intracranial tumors , infections, vascular disorders (aneurysms ) , hypoxia , medications(clonidine ,phencyclidine ). • nephrogenic diabetes insipidus (NDI): -renal insensitivity to normally secrection ADH -familial, drug induced (Li , demeclocycline ), results of hypokalemia ,hypercalcemia , intrinsic renal disease ) • Reset osmostat • Skin losses • Iatrogenic
Disorders of Sodium balance hypernatremia • ECF volume : expanded : hypervolemic hypernatremia : gain of water and sodium : • Iatrogenic : parenteral administration of hypertonic solutions(NaHCO3, saline , medications and nutrition ) • Mineralocorticoid excess
Disorders of Sodium balance hypernatremia Treatment: • Water deficit (L)=0.6 x total body weight (kg)x[(serumNa in mmol/L/140)=1] • Rapid correction of hypernatremia can result in cerebral edema , permanent neurological damage • Only one half of the water deficit should be corrected over the first 24 hr , with the remainder being corrected over the follwing 2 to 3 days . • Central diabetes insipidus :treated with desmopressin acetate administrated intranasally [0.1 to 0.4 ml daily ] or subcutaneously or intravenously [0.5 to 1 ml daily ].
Disorders of potassium balance Physiology : • K is the major intracellular cation, with only 2% of total body k located in the extracellular space • The normal serum concentration is 3.3 to 4.9 mmol/L . • Approximately 50 to 100 mmol of k is ingested and absorbed daily , 90% of k is renally excreted with the remainder eliminated in stools.
Disorders of potassium balance Hyperkalemia: • Plasma K+ > 5.5 • Hyperkalemia can result from: 1- Intercompartment shift of K+ ions • in large burns and severe muscle trauma • acidosis, • cell lysis following chemotherapy. • massive tissue trauma • rhabdomyolysis • drugs: digitalis overdose, B2 adrenergic blockage, succinylcholine
Disorders of potassium balance 2. decreasedexcretion of K+ : • Renal failure • K+ sparing diuretic , Spironolactone. • ACE inhibitors • NSAIDs • Cyclosporin.
Disorders of potassium balance 3- Increased K+ intake: • rarely causing hyper K+ in normal individuals unless large amounts are given rapidly by IV. • K+ intake increases in patients receiving B blockers, RF, insulin deficiency will cause hyperkalemia • Unrecognized sources of K+ :include K+ penicillin, K+ salts, transfusion of stored whole blood ( plasma K+ in a unit of whole blood can increase to 30 mEq/L after 21 days of storage).
Disorders of potassium balance Treatment: • Drugs contributing to hyper K+ should be D/C and sources of increased K+ intake should be stopped. • If due to hypoaldosteronism, Rx with mineralocorticoid replacement. • Calcium ( 5 – 10 ml of 10% calcium gluconate or 3 – 5 ml of 10% calcium chloride ) partially antagonizes the cardiac effects of hyper K+ & is useful in marked hyper K+ ( has rapid but short action ).