Download
1 / 1

E N D
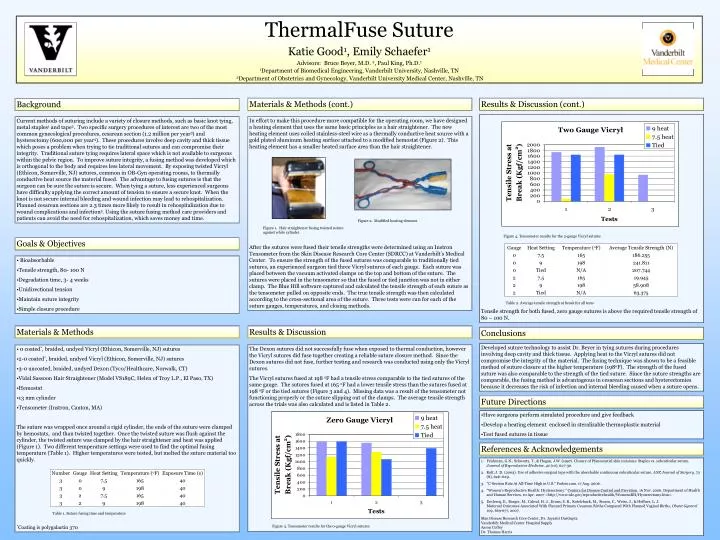
Background Current methods of suturing include a variety of closure methods, such as basic knot tying, metal staples1 and tape2. Two specific surgery procedures of interest are two of the most common gynecological procedures, cesarean section (1.2 million per year3) and hysterectomy (600,000 per year4). These procedures involve deep cavity and thick tissue which poses a problem when trying to tie traditional sutures and can compromise their integrity. Traditional suture tying requires lateral space which is not available to surgeons within the pelvic region. To improve suture integrity, a fusing method was developed which is orthogonal to the body and requires less lateral movement. By exposing twisted Vicryl (Ethicon, Somerville, NJ) sutures, common in OB-Gyn operating rooms, to thermally conductive heat source the material fused. The advantage to fusing sutures is that the surgeon can be sure the suture is secure. When tying a suture, less experienced surgeons have difficulty applying the correct amount of tension to ensure a secure knot. When the knot is not secure internal bleeding and wound infection may lead to rehospitalization. Planned cesarean sections are 2.3 times more likely to result in rehospitalization due to wound complications and infection5. Using the suture fusing method care providers and patients can avoid the need for rehospitalization, which saves money and time. Figure 2. Modified heating element. Figure 1. Hair straightener fusing twisted suture against white cylinder. Goals & Objectives • Bioabsorbable • Tensile strength, 80- 100 N • Degradation time, 3- 4 weeks • Unidirectional tension • Maintain suture integrity • Simple closure procedure Figure 3. Tensometer results for the 0-gauge Vicryl sutures Figure 4. Tensometer results for the 2-gauge Vicryl sutures ThermalFuse Suture Katie Good1, Emily Schaefer1 Advisors: Bruce Beyer, M.D. 2, Paul King, Ph.D.1 1Department of Biomedical Engineering, Vanderbilt University, Nashville, TN 2Department of Obstetrics and Gynecology, Vanderbilt University Medical Center, Nashville, TN Materials & Methods (cont.) Results & Discussion (cont.) Tensile strength for both fused, zero gauge sutures is above the required tensile strength of 80 – 100 N. In effort to make this procedure more compatible for the operating room, we have designed a heating element that uses the same basic principles as a hair straightener. The new heating element uses coiled stainless-steel wire as a thermally conductive heat source with a gold plated aluminum heating surface attached to a modified hemostat (Figure 2). This heating element has a smaller heated surface area than the hair straightener. After the sutures were fused their tensile strengths were determined using an Instron Tensometer from the Skin Disease Research Core Center (SDRCC) at Vanderbilt’s Medical Center. To ensure the strength of the fused sutures was comparable to traditionally tied sutures, an experienced surgeon tied three Vicryl sutures of each gauge. Each suture was placed between the vacuum activated clamps on the top and bottom of the suture. The sutures were placed in the tensometer so that the fused or tied junction was not in either clamp. The Blue Hill software captured and calculated the tensile strength of each suture as the tensometer pulled on opposite ends. The true tensile strength was then calculated according to the cross-sectional area of the suture. Three tests were run for each of the suture gauges, temperatures, and closing methods. Table 2. Average tensile strength at break for all tests Materials & Methods Results & Discussion Conclusions Developed suture technology to assist Dr. Beyer in tying sutures during procedures involving deep cavity and thick tissue. Applying heat to the Vicryl sutures did not compromise the integrity of the material. The fusing technique was shown to be a feasible method of suture closure at the higher temperature (198oF). The strength of the fused suture was also comparable to the strength of the tied suture. Since the suture strengths are comparable, the fusing method is advantageous in cesarean sections and hysterectomies because it decreases the risk of infection and internal bleeding caused when a suture opens. The Dexon sutures did not successfully fuse when exposed to thermal conduction, however the Vicryl sutures did fuse together creating a reliable suture closure method. Since the Dexon sutures did not fuse, further testing and research was conducted using only the Vicryl sutures. The Vicryl sutures fused at 198 oF had a tensile stress comparable to the tied sutures of the same gauge. The sutures fused at 165 oF had a lower tensile stress than the sutures fused at 198 oF or the tied sutures (Figure 3 and 4). Missing data was a result of the tensometer not functioning properly or the suture slipping out of the clamps. The average tensile strength across the trials was also calculated and is listed in Table 2. • 0 coated*, braided, undyed Vicryl (Ethicon, Somerville, NJ) sutures • 2-0 coated*, braided, undyed Vicryl (Ethicon, Somerville, NJ) sutures • 3-0 uncoated, braided, undyed Dexon (Tyco/Healthcare, Norwalk, CT) • Vidal Sassoon Hair Straightener (Model VS189C, Helen of Troy L.P., El Paso, TX) • Hemostat • 13 mm cylinder • Tensometer (Instron, Canton, MA) • The suture was wrapped once around a rigid cylinder, the ends of the suture were clamped by hemostats, and than twisted together. Once the twisted suture was flush against the cylinder, the twisted suture was clamped by the hair straightener and heat was applied (Figure 1). Two different temperature settings were used to find the optimal fusing temperature (Table 1). Higher temperatures were tested, but melted the suture material too quickly. • *Coating is polygalactin 370 Future Directions • Have surgeons perform simulated procedure and give feedback • Develop a heating element enclosed in steralizable thermoplastic material • Test fused sutures in tissue References & Acknowledgements • Frishman, G.N., Schwartz, T., & Hogan, J.W. (1997). Closure of Pfannenstiel skin incisions: Staples vs. subcuticular suture. Journal of Reproductive Medicine, 42 (10), 627-30. • Kolt, J. D. (2003). Use of adhesive surgical tape with the absorbable continuous subcuticular suture. ANZ Journal of Surgery, 73 (8), 626–629. • "C-Section Rate At All-Time High in U.S." Forbes.com. 17 Aug. 2006. • "Women's Reproductive Health: Hysterectomy." Centers for Disease Control and Prevetion. 16 Nov. 2006. Department of Health and Human Services. 10 Apr. 2007 <http://www.cdc.gov/reproductivehealth/WomensRH/Hysterectomy.htm>. • Declercq, E., Barger, M., Cabral, H. J., Evans, S. R., Kotelchuck, M., Simon, C., Weiss, J., & Heffner, L. J.Maternal Outcomes Associated With Planned Primary Cesarean Births Compared With Planned Vaginal Births, Obstet Gynecol 109, 669-677, 2007. • Skin Disease Research Core Center, Dr. Jayastri DasGupta • Vanderbilt Medical Center Hospital Supply • Aaron Coffey • Dr. Thomas Harris Table 1. Suture fusing time and temperature