Download
1 / 42
450 likes | 820 Vues
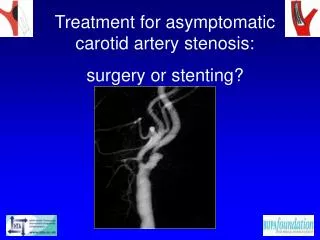
Renal Artery Stenosis: An important cause of hypertension. Dr Claire Hathorn SpR, RHSC Edinburgh 11 th May 2010. Presentation. 3 year old girl Well Minor intercurrent illness – A&E BP 144/91. History & Examination. Asymptomatic PMH – Eczema, viral induced wheeze FH – nil of note

E N D
Renal Artery Stenosis: An important cause of hypertension Dr Claire Hathorn SpR, RHSC Edinburgh 11th May 2010
Presentation • 3 year old girl • Well • Minor intercurrent illness – A&E • BP 144/91
History & Examination • Asymptomatic • PMH – Eczema, viral induced wheeze • FH – nil of note • Normal examination • Height and weight on 97th centile
Initial Investigations • BP 120-140 / 90-100 mmHg • Urinalysis negative • FBC, U&Es, LFTs, coagulation • 4 limb BP • ECG • Renal USS & dopplers • ALL NORMAL
Further Investigations • Renin 2.6 • Aldosterone 136 • Cortisol 192 • PTH 34 • ACTH 12 • Complement 560 • C3 1.01 • C4 0.18 • ANA neg • Urine catecholamines N • Urine cortisol 11.9 • Urine prot:creat ratio 39 (slightly raised) • Urine MC&S negative
Radiology • Echo – normal • DMSA – divided function 50% • MR Angiogram – slight irregularity of superior surface of right renal artery, felt unlikely to represent stenosis. No evidence of duplex. Conclusion: normal.
Specialist Opinions • Cardiology: • No clinical evidence of coarctation • No LVH on Echo • Ophthalmology • Examination normal • No hypertensive retinopathy • No cause or complication of hypertension
Impression & Management • Blood pressure not well-controlled on 3 drugs • Atenolol 20mg bd • Amlodipine 2.5mg od • Doxazosin 0.5mg od • Renovascular disease most likely diagnosis • Referred for formal angiography at Great Ormond Street Hospital
Angiography • Critical stenosis of left upper pole branch of main renal artery • Normal right renal arteries • Angioplasty performed • Atenolol & Doxazosin stopped • Aspirin started
Progress • Remained hypertensive 1 month post-angioplasty: 120/61 • Amlodipine continued • Doxazosin restarted • 3 months post-angioplasty, BP well-controlled: 50-75th centile
Renovascular Hypertension • Aetiology • Clinical Features • Investigations • Management
Renovascular Hypertension • 5-10% of all childhood hypertension • Amenable to potentially curative treatment • Causes & management different to adults
Aetiology in Children • Fibromuscular dysplasia – most common in UK • Syndromes: Neurofibromatosis, Williams, Marfan • Vasculitides: Takayasu, Kawasaki • Extrinsic compression: Wilm’s, Neuroblastoma • Other: Renal transplant, trauma, radiation
Clinical Spectrum • Bilateral disease in 53-78% • Intrarenal disease in 44% • Intrarenal & main artery stenosis in 31% • Most children without co-morbidities have single focal branch artery stenosis Tullus et al. Renovascular hypertension in children. Lancet. 2008;371:1453-1463
Anatomic distribution of renal artery stenosis in children: implications for imaging • Cinncinnati Children’s Hospital, 1993-2005 • 24 stenoses identified in 21 children, R=L • 12 male, mean age 9yrs 3mths (30 mths – 18 yrs) • No co-morbidities • 90% children had a single stenosis • 75% lesions located in branch / accessory arteries Vo et al. Pediatric Radiology 2006;36:1032
Clinical Features Schroff et al. Angioplasty for renovascular hypertension in children: 20 year experience. Pediatrics 2006;118:268-275
Renovascular disease and more widespread arterial involvement
Implications of widespread arterial disease • Improved BP control • 11/13 (85%) isolated RAS • 6/20 (30%) associated intra or extra renal disease • Recommend routine cerebrovascular imaging • MR / PET scanning Schroff et al. Angioplasty for renovascular hypertension in children: 20 year experience. Pediatrics2006;118:268-275
Investigation • Doppler ultrasound • Measurement of plasma renin activity • Captopril plasma renin test • Renal vein sampling • Scintigraphy: DMSA or MAG3 • CT & MR angiography • Angiography: Gold Standard
DMSA scintigraphy before & after Captopril Tullus et al. Renovascular hypertension in children. Lancet. 2008;371:1453-1463
CT Angiogram Tullus et al. Renovascular hypertension in children. Lancet. 2008;371:1453-1463
Angiography • With carefully selected patients, 40% RAS • Important therapeutic opportunity • Visualisation of abdominal vessels
Angiography: Indications • Tulles et al. (2008) • BP >95th centile not well-controlled on 2 drugs • Other cause not identified • Vo et al. (2006) • Unexplained persistent HT > 95th centile • Shahdadpuri et al. (2000) • BP > 99th centile not controlled with 1 drug • Angiography abnormal in 43% patients
A 4-year-old hypertensive boy Vo et al. Anatomic distribution of RAS in children. Pediatric Radiology 2006;36:1032
14 yr old hypertensive girl Vo et al. Anatomic distribution of RAS in children. Pediatric Radiology 2006;36:1032
Medical Management • Anti-hypertensives • Multiple often required • Adequate BP control often not possible • Adverse effects common • Avoid ACE inhibitors & angiotensin receptor blockers • Concern re renal function if BP well-controlled due to under-perfusion of kidneys
Angioplasty • 1980 : 1st successful angioplasty in a child • Balloon diameter equal to proximal artery • Stent if residual diameter stenosis <50% • Complications • Arterial spasm • Dissection • Arterial rupture • Post-procedure: Aspirin 3-6 months Tullus et al. Renovascular hypertension in children. Lancet. 2008;371:1453-1463
Angioplasty for renovascular hypertension in children: 20 year experience • Retrospective review from GOS • All children undergoing PTA 1984-2003 • Only stenoses in main or large segmental arteries • Excluded transplants & inflammatory disorders • 33 children, 1.9-17.9 yrs (median 10.3) • 10 with underlying syndromes • 16 bilateral RAS • 15 intrarenal disease • 48 procedures, including 15 stents Schroff et al. Pediatrics 2006;118:268-275
Angioplasty for renovascular hypertension in children: 20 year experience • Final outcomes of PTA: • 18 (55%) improved BP control • 11/13 (85%) if isolated main RAS • 10 (30%) ongoing HT despite adequate dilation • 5 (15%) PTA unsuccessful • Restenosis in 2/27 native renal arteries after balloon dilatation, 7/19 of stented arteries • 6 (18%) suffered complications, incl 1 death Schroff et al. Pediatrics 2006;118:268-275
Left RAS before & after Angioplasty Schroff et al. Angioplasty for renovascular hypertension in children: 20 year experience. Pediatrics 2006;118:268-275
Surgery • For refractory HT when medical Rx & angioplasty have failed • Nephrectomy • Revascularisation procedures • Aortic reconstruction
Results of surgical treatment for RVH in children: 30 yr single centre experience • 37 children (65% male) • 1979 - 2008 • Mean SBP 140 (105-300) mmHg • 53 surgical procedures • Nephrectomy 18 • Renovascular surgery 28 • Aortic reconstruction 7 Stadermann et al. Nephrology Dialysis Transplantation. 2010;25(3):807-813
Results of surgical treatment for RVH in children: 30 yr single centre experience • 12 months post-op: • 16 (43%) normal BP without treatment • 15 (41%) normal/improved BP on 1-4 drugs • 4 (11%) unchanged • 90% overall improvement • Complications: • Haemorrhage (5) • Septicaemia (5) • Chylous ascites (1) Stadermann et al. Nephrology Dialysis Transplantation. 2010;25(3):807-813
Children not amenable to Angioplasty or Surgery • Diffuse abnormalities of very small intrarenal arteries • Antihypertensive medication • Uncontrolled on 6-7 drugs not uncommon • Therapeutic trial with ACE inhibitor or angiotensin blocker warranted Tullus et al. Renovascular hypertension in children. Lancet. 2008;371:1453-1463
Tullus et al. Renovascular hypertension in children. Lancet. 2008;371:1453-1463
Our Patient • 3 months post-angioplasty • BP well-controlled on 2 drugs • Close follow-up • BP • Renal function • DMSA • ? Consider cerebrovascular imaging