Download
1 / 23
250 likes | 418 Vues
Chapter 14 Organization and control of circulation to skeletal mucsle. Introduction. Blood flow in microcirculation Degree to which muscle blood flow can increase Relationship between metabolism, blood flow and Vo 2 Coupling between skeletal muscle and vascular supply Role of SNS.

E N D
Chapter 14Organization and control of circulation to skeletal mucsle
Introduction • Blood flow in microcirculation • Degree to which muscle blood flow can increase • Relationship between metabolism, blood flow and Vo2 • Coupling between skeletal muscle and vascular supply • Role of SNS
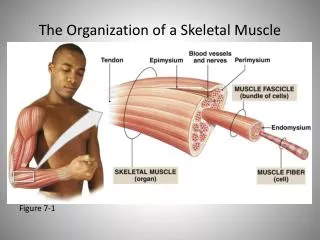
Organization and control of circulation to skeletal muscle • Conduit arteries: • Large, act like pipes to convey large amounts of blood to areas in bulk • Feed arteries: • Muscular, act as resistance vessels • Constrict or dilate to control blood flow into microvascular networks • Both are external to muscle • Not directly responsive to vasoactive stimuli produced within muscle fibers
Organization and control of circulation to skeletal muscle • Primary arterioles: • Within skeletal muscle • Branch into 2cd and 3rd order arterioles • Distribute blood within muscle • 4th order and terminal arterioles • Control perfusion of capillaries • Collecting venules • Receive effluent blood from capillary bed • These empty into progressively larger venules Arteriolar diameter: 10-100 μm
Resistance vessels • Arteriolar control of blood flow • Smooth muscle contraction • VC and VD • Smooth muscle cells encircle arterioles • Capillaries do NOT have smooth muscle • Exchange vessels • While diameter of caps is smallest (maybe 5 μm), there are many of them • Low resistance and high total surface area • Venules • Have smooth muscle • Regulates capacitance of these vessels
Resistance Vessels • Intimal surface • Continuous layer of endothelial cells (50-100 microns long and 5-10 microns wide) • Direct contact with blood • Smooth muscle and endothelium • Separated by elastic lamina • Sympathetic nerves • Surround feed arteries and arterioles
Capillaries: microvascular units • Microvascular unit • All the caps that arise from a given terminal arteriole • TA’s run perpendicular to fiber, to caps run along fiber • About 1 mm in length • Maybe 20 caps arise from each TA • Cover about 0.1 mm3 • Each MVU supplies 20-30 fibers
Capillaries: muscle fiber and MVU recruitment • Perfusion is controlled at the level of the TA • Constriction: shuts off MVU • Dilation: opens MVU • RBC distribution within MVU • Not uniform • Determined in part by metabolism of contraction fibers and hemodynamics
Muscle fiber-MVU relationships • Muscle fibers are several cm long (order of magnitude longer than MVU) • Multiple MVUs supply each fiber • Muscle fibers of a motor unit are dispersed within muscle (not spatially organized) • Thus, firing of a motor unit will result in the perfusion of more MVUs than needed (particularly at low levels of recruitment) • Flow is both concurrent and counter-current • Offsets heterogeneities in O2 delivery within and between fibers
O2 Diffusion: from microvessel to myocyte • Capillary density • Principle determinant • Early thought • Krogh cylinder • Each capillary supplies fibers surrounding it • Theory arose from cross-sectional (2D) analyses • Thus, capillary density (# of caps/mm2) or cap-to-fiber ratio dominated early work • Cap-to-fiber ratio can be constant over training states; how? • 3D models are more insightful • Cap volume per muscle fiber volume • Accounts for tortuosity and branching not noted in 2D modelling
Diffusion • According to Krogh model • Inc in metabolic rate will reduce intracellular Po2 • Increases gradient (PcapO2-PiO2) • At this point, Vo2 is limited by flow through capillary bed • Best, to have many MVUs perfused at onset of contractions
Red Blood Cell Transit Time: determinant of extraction? • Proportional to the length (TA to CV) and inversely proportional to velocity • Transit time • Increased length • Determined by tortuosity, number of caps perfused and RBC spacing • Velocity • Determined by total capillary volume density • However • Blood flow is NOT homogeneous throughout caps • Caps are not straight tubes • Difficult to determine transit time
Altered capillary hematocrit • Capillary hematocrit varies greatly from rest to exercise • Number of RBCs per unit capillary length • May double from rest to exercise (20 to 40%) • Reduces RBC spacing with augments diffusion of O2 • Caused by glycocalyx which retards plasma flow to a greater degree at rest
Oxygen diffuses out of arterioles and between microvessels • Major gradient is between cap and myocyte • Mean cap Po2 20-40 mmHg • Intramyocyte Po2 <5 mmHg • However, may be some cap to cap O2 transfer, particularly betw O2 depleted caps and “fresher” caps • May also be some arteriolar and venular diffusion • Likely small % of total • All these diffusional relations (cap-to-cap; arteriolar-venular) • Likely reduce heterogeneity of O2 delivery to muscle
What determines O2 supply? • Tissue demand clearly results in changing O2 supply • Is there an O2 sensor? • Tissue Po2 varies • Myoglobin tends to smooth this out • Likely that tissue Po2 determines metabolic state of cell • Upstream sensor? • Capillary Po2 • RBC • Likely a combination • Lowered tissue Po2 mandates increased non-aerobic metabolism, which stimulates increased blood flow (baroreceptors, NO-signalling) • This serves to match supply to demand
Blood flow controlled in response to metabolic demand in muscle fibers • Blood flow • Proportional to oxidative capacity • Fiber type • Type of activity • Locomotor muscles vs postural • Diffs in NOS
Meeting demand: Motor unit recruitment promotes capillary perfusion • Muscles fibers larger than microvascular units which supply them • Muscle fibers of a particular motor unit are dispersed throughout muscle • May seem wasteful, but this feed forward type mechanism may prevent large scale supply-demand mismatches • Also, helps explain why adjustment to higher exercise intensities is facilitated by prior warm-up exercise
Ascending Vasodilation • At rest • Resistance is high • Blood flow is low • O2 Extraction is relatively low (~20%) • Exercise • First: increase extraction (extraction reserve) • Fall in intracellular Po2 • Increase in capillary perfusion (dilation of terminal arterioles) • Vasodilations then spreads up the vascular tree • TA, distal arterioles, larger arterioles, feed arteries • These upstream events occur in concert with greater motor unit recruitment
Functional hyperemia • Multiple signals • Vasoconstriction • Inc in free Ca2+ • Voltage-modulated Ca2+ channels • Dependent upon K+ channels • Also intracellular Ca2+ stores (ER) • Second messenger systems (IP3) • Vasodilatory signals • Hyperpolarization • Nitric oxide
Myogenic autoregulation • Increase in wall stress (proportional to transmural pressure X luminal radius and inversely proportional to wall thickness) • Stimulate smooth muscle contraction • Maintains constancy of tissue blood flow • During muscular contractions • When muscle relaxes • Reduces transmural pressure and causes vasodilation
Local metabolic vasodilation • Increase in metabolic rate causes the release of vasodilatory substances • These help to match O2 supply and demand • Thus, while SNA and autoregulation will tend to VC areas that are inactive; vasodilatory substances will do the opposite • Potassium • EIHF (ex-induced hyperpolarizing factor) • NO (increased via shear stress) • Adenosine • ALL increase with muscle activity
Muscle pump • Rhythmic changes in intramuscular pressure with dynamic exercise • Veins fill when muscle relaxes • Blood is expelled when muscle contracts • Valves maintain uni-directional flow