Download
1 / 135
1.36k likes | 1.55k Vues
Dislocations. Out of Joint In The ED. Overview. Joint dislocations require prompt and effective care in the Emergency Department Objectives: Discuss several techniques for shoulder reductions Discuss Hip dislocations/reduction Management and complications of knee dislocation

E N D
Dislocations Out of Joint In The ED
Overview • Joint dislocations require prompt and effective care in the Emergency Department • Objectives: • Discuss several techniques for shoulder reductions • Discuss Hip dislocations/reduction • Management and complications of knee dislocation • Elbow dislocations and techniques for reduction • Patellar dislocation
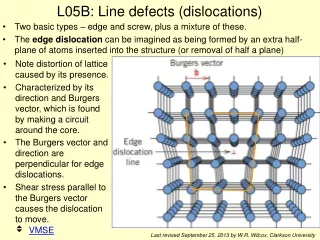
Shoulder Dislocations 50% percent of all major joint dislocations Anterior most common 95-97% Posterior 2-4% Inferior ( luxatio erecta-which means “ to place upward”) Anatomy: shoulder is an inherently unstable joint. Glenoid is shallow-allows for wide range of movement Labrum fibrocartilaginous structure surrounds glenoid inserts into edge of joint capsule
Inferoglenohumeral ligament :anterior/inferior portion of the capsule..thicker than the others and provides strongest support against dislocation • Rotator cuff muscles provide additional support: • subscapularis lies anterior • supraspinatus/infraspinatus/Teres minor • (SITS) lie posterior “pull” humeral head into glenoid
Axillary nerve most commonly injured nerve in shoulder dislocations • Runs inferior to humeral head. • Innervates deltoid, teres minor—Shoulder badge” distribution
Types of Shoulder dislocations • Anterior- majority • subglenoid 30% • subcoracoid 70% • Very rare infraclavicular • Mechanism: usually caused by a blow or force to abducted externally rotated and extended arm… Think blocking a basketball shot • Also fall on outstretched arm
Mechanism of Dislocation • Sports/ trauma ect
Examination • Anterior dislocation arm slightly abducted • Externally rotated .Pt resists all movement. Loss of normal rounded appearance
Typical apperance • Arm abducted/ ext • rotation
Posterior • Less common 3-5 % • May be difficult to diagnose-may miss on up to 50% standard ap view as findings subtle • Commonly assoc with greater tuberosity/surgical neck fx’s can cause a reverse hills sachs deformity • If plain X rays indeterminate can use CT • CT also aids ortho as to who needs OR • As % articular surface involved changes care
Fullness posteriorly. Somewhat squared off shoulder. Marked decreased rom
Helpful radiographic signs • Lightbulb sign-humeral head internally rotated. tuberosity no longer project laterally( circular look to HH) • Rim sign- refers to distance from medial aspect of humeral head to ant glenoid rim • If superimposed or widened joint space >6mm • Suspect post dislocation
Trough line sign • 2 parallel lines of cortical bone are seen on medial cortex of HH,one line is medial cortex of HH other line is “trough of impaction fx ( reverse hill sachs) anterior articular surface of HH
Mechanism: • electric shock • seizures • trauma ( alchoholics) • Internal rotation/adduction/flexion
Luxatio erecta • Very rare .5 % • Mechanism axial loading foreceful hyperabduction. • Pt falls grasping object above their head • Arm locked in abduction often fore arm resting on head • 60% of pts have some neurologic dysfunction
Neurovascular exam-check distal pulses/axillary nerve function:some dysfunction in 42% of cases( almost all recover) • Cant check deltoid teres minor motor • Can check sensation • Think security guard/ arm forces patch location for axillary
Radial • Dorsal hand sensation web space • Wrist drop
Radiographic evaluation • Excludes fractures/confirms dislocation/confirms reduction • Clinically important fx’s can occur up to 25% • Assoc factors : age >40 • 1st time dislocation • traumatic dislocation • If all 3 absent can safely skip prereduction xray • ( 96% negative prediction value)
Routine films • AP • Scapular Y view • Axillary view
Y view • Beam directed parallel to scapular body. • Y formed by body/spine and the coracoid process. Glenoid fills in center of Y( normally obscured by humeral head ) • With a dislocation Humeral head appears medial to glenoid