Download
1 / 18
180 likes | 256 Vues
Oral Cilostazol Prevents Restenosis And Repeat Revascularization After Percutaneous Coronary Stenting: A Meta-Analysis Of 15 Randomized Trials And 4897 Patients. G. Biondi-Zoccai, 1 C. Moretti, 1 M. Lotrionte, 2 P. Agostoni, 3 F. Sciuto, 1

E N D
Oral Cilostazol Prevents Restenosis And Repeat Revascularization After Percutaneous Coronary Stenting: A Meta-Analysis Of 15 Randomized Trials And 4897 Patients G. Biondi-Zoccai,1 C. Moretti,1 M. Lotrionte,2 P. Agostoni,3 F. Sciuto,1 P. Omedé,1 A. Abbate,4 G. P. Trevi,1 and I. Sheiban1 1University of Turin, Turin, Italy (gbiondizoccai@gmail.com); 2Catholic University, Rome, Italy; 3AZ Middelheim, Antwerp, Belgium; 4Virginia Commonwealth University, Virginia, USA
BACKGROUND • Drug-eluting stents (DES) reduce the risk of restenosis after percutaneous coronary intervention (PCI) in comparison to bare-metal stents (BMS), but may pose a risk of thrombosis. • Furthermore, DES are not uniformly powerful in reducing restenosis, especially in patients with abundant neointimal hyperplasia (eg diabetics).
BACKGROUND • Cilostazol is an oral antiplatelet agent with pleiotropic effects, including inhibition of neointimal hyperplasia. • It is a safe agent, already approved in several countries for the symptomatic treatment of intermittent claudication and peripheral artery disease • Cilostazol could hold the promise of preventing both restenosis and thrombosis after PCI with stenting.
OBJECTIVES • We aimed to systematically review randomized clinical trials on the angiographic and clinical impact of cilostazol after percutaneous coronary stenting. • Our goal was specifically to pool major outcomes from included studies with meta-analytic techniques.
METHODS • We searched Bio-MedCentral, CENTRAL, clinicaltrials.gov, EMBASE, and PubMed for randomized trials comparing cilostazol vs control after PCI (keywords: cilostazol, coronary, and restenosis; updated March 2008). • Inclusion criteria were: (a) randomized allocation, (b) comparison of cilostazol vs control, (c) after PCI with stenting, and (d) follow-up ≥1 month. • Exclusion criteria were: (a) duplicate reports, (b) lack of outcome data beyond hospitalization, and (c) equivocal or nonrandom treatment allocation.
METHODS • Co-primary end-points were binary angiographic restenosis and repeat revascularization, abstracted and pooled by means of random-effect relative risks (RR) with RevMan 4.2 (Cochrane Collaboration). • Stent thrombosis and small study/ publication bias (ie the likelihood of small yet nominally significant studies being selectively published in the literature) were also appraised.
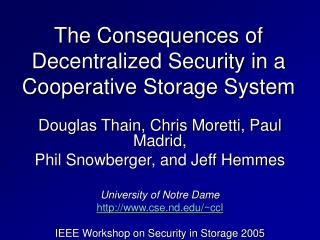
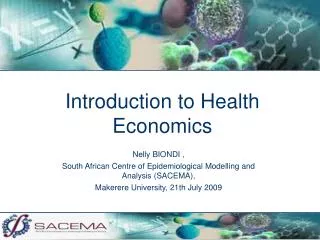
RESULTS • A total of 21 randomized clinical trials were included (5577 patients, 2780 randomized to oral cilostazol for 1-6 months, and 2797 randomized to control therapy or placebo), with median follow-up of 6 months. • Pooled analysis showed that cilostazol was associated with statistically significant reductions in binary angiographic restenosis (relative risk=0.61 [95% confidence interval 0.51-0.75], p<0.001) and repeat revascularization (relative risk=0.73 [0.60-0.88], p=0.001).
RESULTS • Cilostazol appeared also safe, with no significant increase in the risk of stent thrombosis (relative risk=1.27 [0.69-2.35], p=0.45) or bleeding (relative risk=0.73 [0.46-1.17], p=0.19). • Sub-analysis restricted to trials using only DES, including a total of 1137 patients, confirmed that cilostazol lead to significant reductions in binary angiographic restenosis (relative risk=0.54 [0.36-0.79], p=0.002).
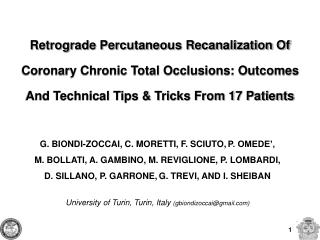
RESULTS • Similarly, among patients treated solely with DES, cilostazol lead to a statistically significant reduction in repeat revascularizations (relative risk=0.47 [0.29-0.76], p=0.002). • Conversely, risk of stent thrombosis or bleeding in DES-treated patients was not significantly influenced by cilostazol (respectively relative risk= 0.77 [0.14-4.06], p=0.76, and relative risk=0.72 [0.23-2.30], P=0.58), . • Funnel plots suggested however the presence of small study bias, but limited to the BMS group.
RISK OF BINARY RESTENOSIS Study Cilostazol Control RR (random) RR (random) or sub-category n/N n/N 95% CI 95% CI 01 BMS Kunishima 3/35 11/41 0.32 [0.10, 1.05] Sekiya 9/82 20/83 0.46 [0.22, 0.94] Yamasaki 0/18 3/17 0.14 [0.01, 2.44] Ochiai 0/23 5/21 0.08 [0.00, 1.42] Park 58/254 65/240 0.84 [0.62, 1.15] Kozuma 10/61 19/58 0.50 [0.25, 0.98] Abe 0/37 15/41 0.04 [0.00, 0.58] Kamishirado 7/54 17/57 0.43 [0.20, 0.97] Mizoguchi 4/65 13/65 0.31 [0.11, 0.89] Inoue 4/34 10/32 0.38 [0.13, 1.08] Sekiguchi 24/89 20/86 1.16 [0.69, 1.94] CREST 57/259 92/267 0.64 [0.48, 0.85] Han 5/34 10/37 0.54 [0.21, 1.43] RACTS 47/202 60/194 0.75 [0.54, 1.04] Takeyasu 119/427 128/436 0.95 [0.77, 1.17] Chen 7/52 17/54 0.43 [0.19, 0.95] Subtotal (95% CI) 1726 1729 0.62 [0.50, 0.78] Total events: 354 (Cilostazol), 505 (Control) Test for heterogeneity: Chi² = 32.08, df = 15 (P = 0.006), I² = 53.2% Test for overall effect: Z = 4.14 (P < 0.0001) 02 DES DECLARE-Long 14/250 23/250 0.61 [0.32, 1.16] CIDES 9/113 20/124 0.49 [0.23, 1.04] DECLARE-DIABETES 13/200 26/200 0.50 [0.26, 0.94] Subtotal (95% CI) 563 574 0.54 [0.36, 0.79] Total events: 36 (Cilostazol), 69 (Control) Test for heterogeneity: Chi² = 0.24, df = 2 (P = 0.89), I² = 0% Test for overall effect: Z = 3.17 (P = 0.002) Total (95% CI) 2289 2303 0.61 [0.51, 0.75] Total events: 390 (Cilostazol), 574 (Control) Test for heterogeneity: Chi² = 34.95, df = 18 (P = 0.010), I² = 48.5% Test for overall effect: Z = 4.86 (P < 0.00001) 0.01 0.1 1 10 100 Favours cilostazol Favours control
RISK OF REPEAT REVASCULARIZATION Study Cilostazol Control RR (random) RR (random) or sub-category n/N n/N 95% CI 95% CI 01 BMS Ochiai 0/25 4/25 0.11 [0.01, 1.96] Park 11/208 13/201 0.82 [0.38, 1.78] Yoon 1/147 1/149 1.01 [0.06, 16.05] Kozuma 15/65 27/65 0.56 [0.33, 0.94] Kamishirado 4/54 12/57 0.35 [0.12, 1.02] Sekiguchi 14/144 11/138 1.22 [0.57, 2.59] CREST 54/354 56/351 0.96 [0.68, 1.35] Han 7/50 11/50 0.64 [0.27, 1.51] Lee 5/344 4/345 1.25 [0.34, 4.63] RACTS 46/201 64/196 0.70 [0.51, 0.97] Takeyasu 96/427 103/436 0.95 [0.75, 1.21] Chen 3/60 10/60 0.30 [0.09, 1.04] Subtotal (95% CI) 2079 2073 0.79 [0.65, 0.96] Total events: 256 (Cilostazol), 316 (Control) Test for heterogeneity: Chi² = 13.82, df = 11 (P = 0.24), I² = 20.4% Test for overall effect: Z = 2.42 (P = 0.02) 02 DES DECLARE-Long 9/250 18/250 0.50 [0.23, 1.09] CIDES 7/141 15/139 0.46 [0.19, 1.09] DECLARE-DIABETES 7/200 16/200 0.44 [0.18, 1.04] Subtotal (95% CI) 591 589 0.47 [0.29, 0.76] Total events: 23 (Cilostazol), 49 (Control) Test for heterogeneity: Chi² = 0.05, df = 2 (P = 0.97), I² = 0% Test for overall effect: Z = 3.09 (P = 0.002) Total (95% CI) 2670 2662 0.73 [0.60, 0.88] Total events: 279 (Cilostazol), 365 (Control) Test for heterogeneity: Chi² = 18.67, df = 14 (P = 0.18), I² = 25.0% Test for overall effect: Z = 3.24 (P = 0.001) 0.01 0.1 1 10 100 Favours cilostazol Favours control
RISK OF STENT THROMBOSIS Study Cilostazol Control RR (random) RR (random) or sub-category n/N n/N 95% CI 95% CI 01 BMS Kunishima 0/30 1/40 0.44 [0.02, 10.46] Sekiya 0/63 3/63 0.14 [0.01, 2.71] Park 2/247 1/243 1.97 [0.18, 21.56] Yoon 1/147 1/149 1.01 [0.06, 16.05] Kozuma 0/62 1/62 0.33 [0.01, 8.03] Kamishirado 0/65 2/65 0.20 [0.01, 4.09] Inoue 0/34 0/32 Not estimable Sekiguchi 8/144 1/138 7.67 [0.97, 60.50] CREST 1/354 1/351 0.99 [0.06, 15.79] Han 1/50 0/50 3.00 [0.13, 71.92] Lee 5/344 4/345 1.25 [0.34, 4.63] RACTS 2/201 2/196 0.98 [0.14, 6.85] Takeyasu 8/321 1/321 8.00 [1.01, 63.59] Subtotal (95% CI) 2062 2055 1.37 [0.70, 2.68] Total events: 28 (Cilostazol), 18 (Control) Test for heterogeneity: Chi² = 11.15, df = 11 (P = 0.43), I² = 1.3% Test for overall effect: Z = 0.92 (P = 0.36) 02 DES DECLARE-Long 1/250 1/250 1.00 [0.06, 15.90] CIDES 1/113 1/124 1.10 [0.07, 17.34] DECLARE-DIABETES 0/200 1/200 0.33 [0.01, 8.13] Subtotal (95% CI) 563 574 0.77 [0.14, 4.06] Total events: 2 (Cilostazol), 3 (Control) Test for heterogeneity: Chi² = 0.36, df = 2 (P = 0.83), I² = 0% Test for overall effect: Z = 0.31 (P = 0.76) Total (95% CI) 2625 2629 1.27 [0.69, 2.35] Total events: 30 (Cilostazol), 21 (Control) Test for heterogeneity: Chi² = 11.93, df = 14 (P = 0.61), I² = 0% Test for overall effect: Z = 0.76 (P = 0.45) 0.001 0.01 0.1 1 10 100 1000 Favours cilostazol Favours control
RISK OF BLEEDING Study Cilostazol Control RR (random) RR (random) or sub-category n/N n/N 95% CI 95% CI 01 BMS Kunishima 0/30 0/40 Not estimable Sekiya 0/63 0/63 Not estimable Ochiai 0/25 0/25 Not estimable Park 2/247 3/243 0.66 [0.11, 3.89] Yoon 2/147 3/149 0.68 [0.11, 3.99] Kamishirado 0/65 1/65 0.33 [0.01, 8.03] Inoue 0/34 0/32 Not estimable Sekiguchi 3/144 1/138 2.88 [0.30, 27.31] CREST 13/354 16/351 0.81 [0.39, 1.65] Han 1/50 2/50 0.50 [0.05, 5.34] Lee 3/344 5/345 0.60 [0.14, 2.50] RACTS 0/201 3/196 0.14 [0.01, 2.68] Takeyasu 1/321 1/321 1.00 [0.06, 15.92] Subtotal (95% CI) 2025 2018 0.73 [0.44, 1.22] Total events: 25 (Cilostazol), 35 (Control) Test for heterogeneity: Chi² = 3.18, df = 8 (P = 0.92), I² = 0% Test for overall effect: Z = 1.19 (P = 0.24) 02 DES DECLARE-Long 2/250 4/250 0.50 [0.09, 2.71] DECLARE-DIABETES 3/200 3/200 1.00 [0.20, 4.90] Subtotal (95% CI) 450 450 0.72 [0.23, 2.30] Total events: 5 (Cilostazol), 7 (Control) Test for heterogeneity: Chi² = 0.34, df = 1 (P = 0.56), I² = 0% Test for overall effect: Z = 0.55 (P = 0.58) Total (95% CI) 2475 2468 0.73 [0.46, 1.17] Total events: 30 (Cilostazol), 42 (Control) Test for heterogeneity: Chi² = 3.53, df = 10 (P = 0.97), I² = 0% Test for overall effect: Z = 1.31 (P = 0.19) 0.001 0.01 0.1 1 10 100 1000 Favours cilostazol Favours control
FUNNEL PLOT FOR BINARY RESTENOSIS 0.0 DES BMS 0.4 0.8 Standard error (log relative risk 1.2 1.6 0.01 0.1 1 10 100 Relative risk (fixed effect)
CONCLUSIONS • Cilostazol appears effective and safe in reducing the risk of restenosis and repeat revascularization after stenting implantation, in both the bare metal and DES era. • This inexpensive treatment can be envisaged in most patients treated with BMS, and in those treated with DES who remain at higher risk of restenosis and thus can benefit from further inhibition of neointimal hyperplasia.
For further slides on these topics please feel free to visit the metcardio.org website:http://www.metcardio.org/slides.html